

A randomized physiotherapy trial in patients with fecal incontinence: design of the PhysioFIT-study
- PMID: 18096041
- PMCID: PMC2234416
- DOI: 10.1186/1471-2458-7-355
A randomized physiotherapy trial in patients with fecal incontinence: design of the PhysioFIT-study
Abstract
Background: Fecal incontinence (FI) is defined as the recurrent involuntary excretion of feces in inappropriate places or at inappropriate times. It is a major and highly embarrassing health care problem which affects about 2 to 24% of the adult population. The prevalence increases with age in both men and women. Physiotherapy interventions are often considered a first-line approach due to its safe and non-invasive nature when dietary and pharmaceutical treatment fails or in addition to this treatment regime. Two physiotherapy interventions, rectal balloon training (RBT) and pelvic floor muscle training (PFMT) are widely used in the management of FI. However, their effectiveness remains uncertain since well-designed trials on the effectiveness of RBT and PFMT versus PFMT alone in FI have never been published.
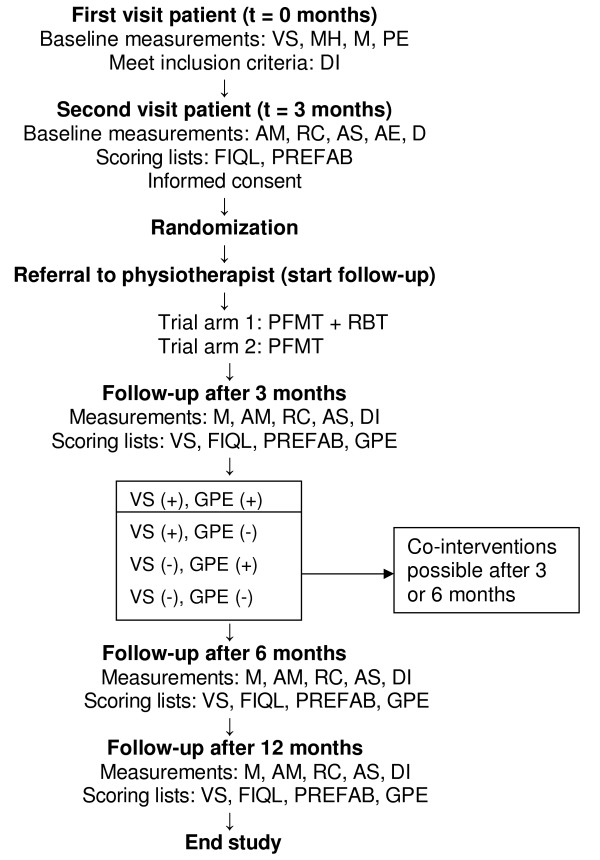
Methods/design: A two-armed randomized controlled clinical trial will be conducted. One hundred and six patients are randomized to receive either PFMT combined with RBT or PFMT alone. Physicians in the University Hospital Maastricht include eligible participants. Inclusion criteria are (1) adults (aged > or = 18 years), (2) with fecal incontinence complaints due to different etiologies persisting for at least six months, (3) having a Vaizey incontinence score of at least 12, (4) and failure of conservative treatment (including dietary adaptations and pharmacological agents). Baseline measurements consist of the Vaizey incontinence score, medical history, physical examination, medication use, anorectal manometry, rectal capacity measurement, anorectal sensation, anal endosonography, defecography, symptom diary, Fecal Incontinence Quality of Life scale (FIQL) and the PREFAB-score. Follow-up measurements are scheduled at three, six and 12 months after inclusion. Skilled and registered physiotherapists experienced in women's health perform physiotherapy treatment. Twelve sessions are administered during three months according to a standardized protocol.
Discussion: This section discusses the decision to publish a trial protocol, the actions taken to minimize bias and confounding in the design, explains the choice for two treatment groups, discusses the secondary goals of this study and indicates the impact of this trial on clinical practice.
Trial registration: The Netherlands Trial Register ISRCTN78640169.
Figures
Similar articles
-
Rectal balloon training as add-on therapy to pelvic floor muscle training in adults with fecal incontinence: a randomized controlled trial.Neurourol Urodyn. 2012 Jan;31(1):132-8. doi: 10.1002/nau.21218. Epub 2011 Oct 28. Neurourol Urodyn. 2012. PMID: 22038680 Clinical Trial.
-
Efficacy of Supervised Pelvic Floor Muscle Training and Biofeedback vs Attention-Control Treatment in Adults With Fecal Incontinence.Clin Gastroenterol Hepatol. 2019 Oct;17(11):2253-2261.e4. doi: 10.1016/j.cgh.2018.12.015. Epub 2018 Dec 20. Clin Gastroenterol Hepatol. 2019. PMID: 30580089 Clinical Trial.
-
Electrical stimulation and pelvic floor muscle training with biofeedback in patients with fecal incontinence: a cohort study of 281 patients.Dis Colon Rectum. 2006 Aug;49(8):1149-59. doi: 10.1007/s10350-006-0569-3. Dis Colon Rectum. 2006. PMID: 16773492
-
Biofeedback for pelvic floor muscle training in women with stress urinary incontinence: a systematic review with meta-analysis.Physiotherapy. 2019 Mar;105(1):10-23. doi: 10.1016/j.physio.2018.07.012. Epub 2018 Sep 24. Physiotherapy. 2019. PMID: 30686479
-
Pelvic Floor Muscle Training Versus Watchful Waiting and Pelvic Floor Disorders in Postpartum Women: A Systematic Review and Meta-analysis.Female Pelvic Med Reconstr Surg. 2018 Mar/Apr;24(2):142-149. doi: 10.1097/SPV.0000000000000513. Female Pelvic Med Reconstr Surg. 2018. PMID: 29474288
Cited by
-
Pelvic floor rehabilitation to improve functional outcome and quality of life after surgery for rectal cancer: study protocol for a randomized controlled trial (FORCE trial).Trials. 2020 Jan 28;21(1):112. doi: 10.1186/s13063-019-4043-7. Trials. 2020. PMID: 31992358 Free PMC article.
-
Pelvic floor physical therapy in the treatment of chronic anal fissure (PAF-study): Study protocol for a randomized controlled trial.Contemp Clin Trials Commun. 2021 Nov 16;24:100874. doi: 10.1016/j.conctc.2021.100874. eCollection 2021 Dec. Contemp Clin Trials Commun. 2021. PMID: 34841124 Free PMC article.
-
Randomised controlled trial to assess efficacy of pelvic floor muscle training on bowel symptoms after low anterior resection for rectal cancer: study protocol.BMJ Open. 2021 Jan 22;11(1):e041797. doi: 10.1136/bmjopen-2020-041797. BMJ Open. 2021. PMID: 33483444 Free PMC article.
-
Improving biofeedback for the treatment of fecal incontinence in women: implementation of a standardized multi-site manometric biofeedback protocol.Neurogastroenterol Motil. 2017 Jan;29(1):10.1111/nmo.12906. doi: 10.1111/nmo.12906. Epub 2016 Jul 24. Neurogastroenterol Motil. 2017. PMID: 27453154 Free PMC article. Clinical Trial.
-
Responsiveness and interpretability of incontinence severity scores and FIQL in patients with fecal incontinence: a secondary analysis from a randomized controlled trial.Int Urogynecol J. 2013 Mar;24(3):469-78. doi: 10.1007/s00192-012-1886-9. Epub 2012 Jul 18. Int Urogynecol J. 2013. PMID: 22806487 Clinical Trial.
References
-
- Johanson JF, Lafferty J. Epidemiology of fecal incontinence: the silent affliction. Am J Gastroenterol. 1996;91:33–36. - PubMed
-
- Perry S, Shaw C, McGrother C, Matthews RJ, Assassa RP, Dallosso H, Williams K, Brittain KR, Azam U, Clarke M, Jagger C, Mayne C, Castleden CM. Prevalence of faecal incontinence in adults aged 40 years or more living in the community. Gut. 2002;50:480–484. doi: 10.1136/gut.50.4.480. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
