

Intra-arrest cooling with delayed reperfusion yields higher survival than earlier normothermic resuscitation in a mouse model of cardiac arrest
- PMID: 18096292
- PMCID: PMC2391241
- DOI: 10.1016/j.resuscitation.2007.10.015
Intra-arrest cooling with delayed reperfusion yields higher survival than earlier normothermic resuscitation in a mouse model of cardiac arrest
Abstract
Background: Therapeutic hypothermia (TH) represents an important method to attenuate post-resuscitation injury after cardiac arrest. Laboratory investigations have suggested that induction of hypothermia before return of spontaneous circulation (ROSC) may confer the greatest benefit. We hypothesized that a short delay in resuscitation to induce hypothermia before ROSC, even at the expense of more prolonged ischemia, may yield both physiological and survival advantages.
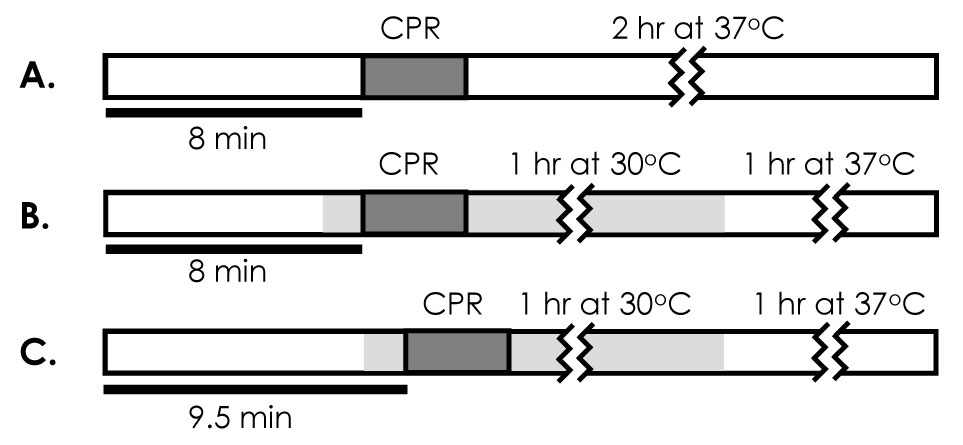
Methods: Cardiac arrest was induced in C57BL/6 mice using intravenous potassium chloride; resuscitation was attempted with CPR and fluid administration. Animals were randomized into three groups (n=15 each): a normothermic control group, in which 8 min of arrest at 37 degrees C was followed by resuscitation; an early intra-arrest hypothermia group, in which 6.5 min of 37 degrees C arrest were followed by 90s of cooling, with resuscitation attempted at 30 degrees C (8 min total ischemia); and a delayed intra-arrest hypothermia group, with 90s cooling begun after 8 min of 37 degrees C ischemia, so that animals underwent resuscitation at 9.5 min.
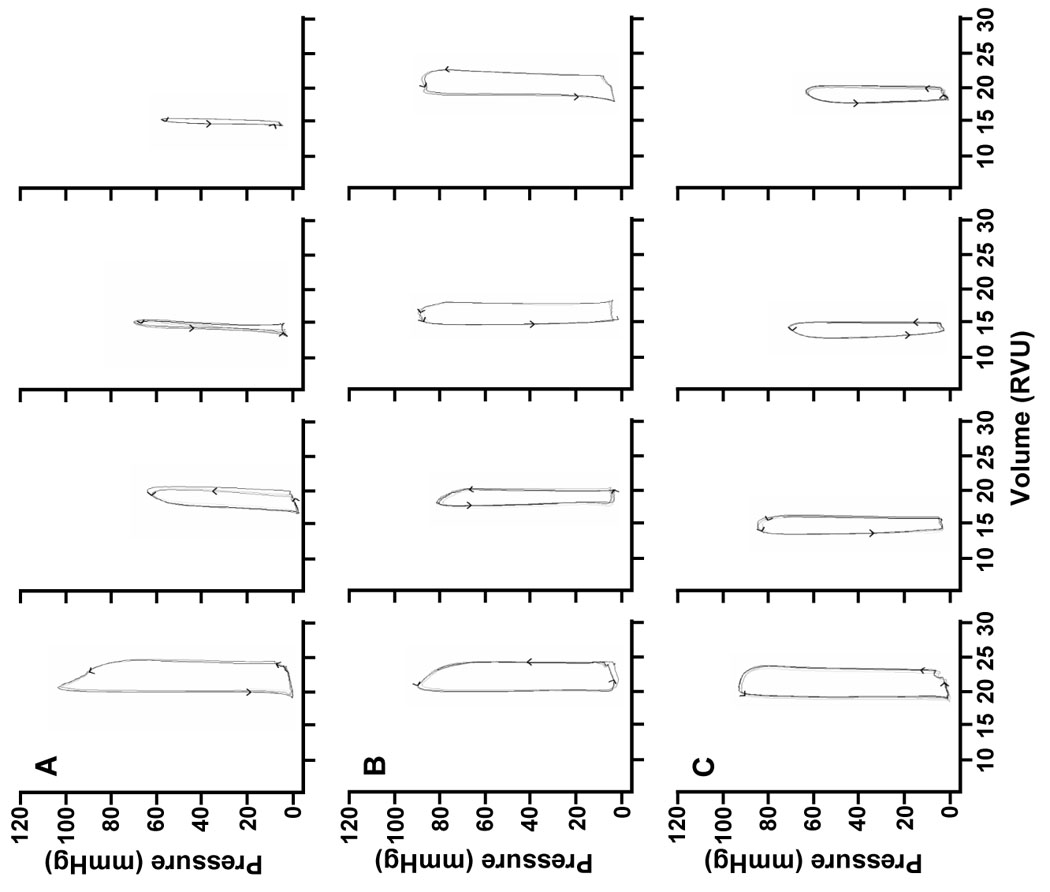
Results: Animals treated with TH demonstrated improved hemodynamic variables and survival compared to normothermic controls. This was the case even when comparing the delayed intra-arrest hypothermia group with prolonged ischemia time against normothermic controls with shorter ischemia time (7-day survival, 4/15 vs. 0/15, p<0.001).
Conclusions: Short resuscitation delays to allow establishment of hypothermia before ROSC appear beneficial to both cardiac function and survival. This finding supports the concept that post-resuscitation injury processes begin immediately after ROSC, and that intra-arrest cooling may serve as a useful therapeutic approach to improve survival.
Conflict of interest statement
Figures



References
-
- 2005 International Consensus on Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care (ECC) Science With Treatment Recommendations. Circulation. 2005;112 suppl III:III-1–III-136.
-
- Eckstein M, Stratton SJ, Chan LS. Cardiac Arrest Resuscitation Evaluation in Los Angeles: CARE-LA. Ann Emerg Med. 2005;45:504–509. - PubMed
-
- Dunne RB, Compton S, Zalenski RJ, Swor R, Welch R, Bock BF. Outcomes from out-of-hospital cardiac arrest in Detroit. Resuscitation. 2007;72:59–65. - PubMed
-
- Hachimi-Idrissi S, Corne L, Ebinger G, Michotte Y, Huyghens L. Mild hypothermia induced by a helmet device: a clinical feasibility study. Resuscitation. 2001;51:275–281. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, Smith K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
