

Functional analysis of swallowing outcomes after supracricoid partial laryngectomy
- PMID: 18098304
- PMCID: PMC4012760
- DOI: 10.1002/hed.20738
Functional analysis of swallowing outcomes after supracricoid partial laryngectomy
Abstract
Background: In this study, we analyzed swallowing recovery after supracricoid partial laryngectomy (SCPL).
Methods: We retrospectively reviewed 27 patients treated with SCPL (September 1997 to March 2005). We evaluated recovery course, nutritional outcomes, and swallowing using objective analysis. Modified barium swallow (MBS) study results identified swallowing physiology and therapeutic effectiveness.
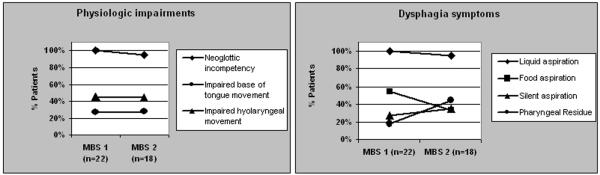
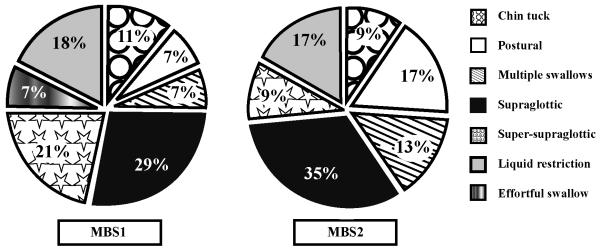
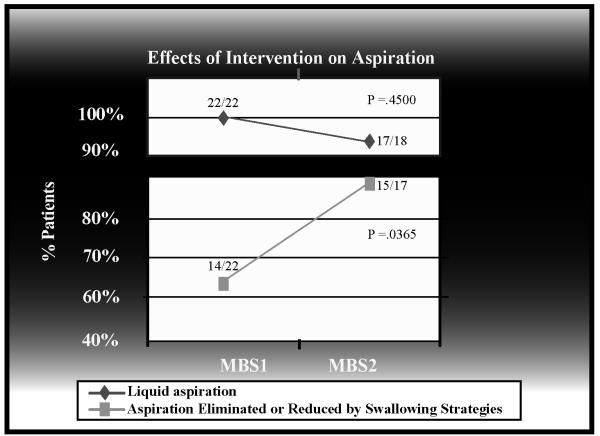
Results: Average length of hospitalization was 7.7+/-9.2 days; time to decannulation was 5.3+/-8.2 weeks. The most common complications included pneumonia and subcutaneous emphysema (26%). Twenty-two patients had MBS studies, in which initially, all patients aspirated due to neoglottic incompetency, and impaired base of tongue and laryngeal movements. Although aspiration rates did not change significantly over time, use of appropriately selected swallowing strategies effectively protected the airway (p= .0365). Ultimately, 81% of patients returned to complete oral intake with median tube removal at 9.4 weeks.
Conclusion: SCPL produces severe dysphagia initially. Our findings suggest that objective swallowing assessment is important for return to oral nutrition after SCPL.
Figures
References
-
- Kotz T, Costello R, Li Y, Posner MR. Swallowing dysfunction after chemoradiation for advanced squamous cell carcinoma of the head and neck. Head Neck. 2004;26:365–72. - PubMed
-
- Mittal BB, Pauloski BR, Haraf DJ. Swallowing dysfunction—preventative and rehabilitation strategies in patients with head-and-neck cancers treated with surgery, radiotherapy, and chemotherapy: a critical review. Int J Radiation Oncology Biol Phys. 2003;57:1219–30. - PubMed
-
- DeSanto LW, Olsen KD, Perry WC, Rohe DE, et al. Quality of life after surgical treatment of cancer of the larynx. Ann Otol Rhinol Laryngol. 1995;104:763–769. - PubMed
-
- Lefebvre JL, Lartigau E. Preservation of form and function during management of cancer of the larynx and hypopharynx. World J Surg. 2003;27:811–816. - PubMed
-
- Weinstein GS, Laccourreye O, Ruiz C. Larynx preservation with supracricoid partial laryngectomy with cricohyoidoepiglottopexy. Ann Otol Rhinol Laryngol. 2002;111:1–7. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
