

Effects of Parkinson's disease and levodopa on functional limits of stability
- PMID: 18155331
- PMCID: PMC2776044
- DOI: 10.1016/j.clinbiomech.2007.11.007
Effects of Parkinson's disease and levodopa on functional limits of stability
Abstract
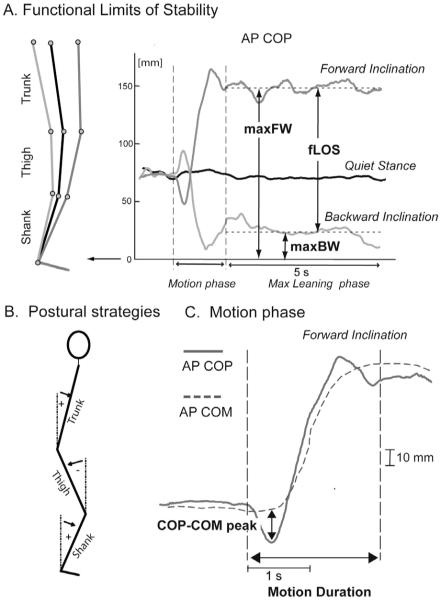
Background: The voluntary, maximum inclined posture reflects the self-perceived limits of stability. Parkinson's disease is associated with small, bradykinetic postural weight shifts while standing but it is unclear whether this is due to reduced limits of stability and/or to the selection of abnormal strategies for leaning. The aim of this study was to investigate the effects of Parkinson's disease and levodopa medication on voluntary limits of stability and strategies used to reach these limits.
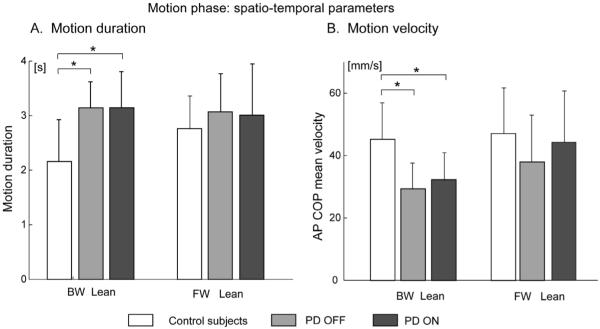
Methods: Fourteen subjects with Parkinson's disease (OFF and ON levodopa) and 10 age-matched controls participated in the study. Functional limits of stability were quantified as the maximum center of pressure excursion during voluntary forward and backward leaning. Postural strategies to achieve functional limits of stability were assessed by (i) body segments alignment, (ii) the difference between center of pressure and center of mass in preparation for a lean, (iii) the timing and the velocity of the preparation phase.
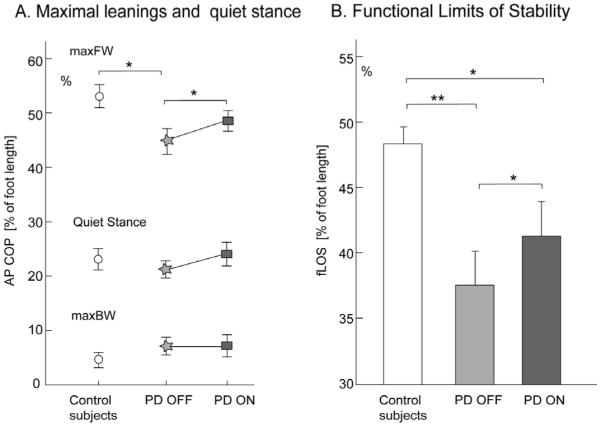
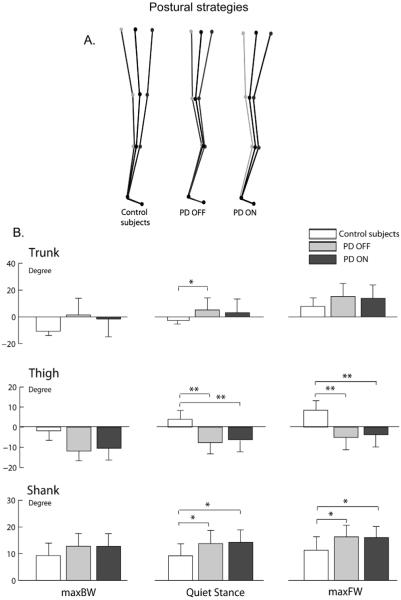
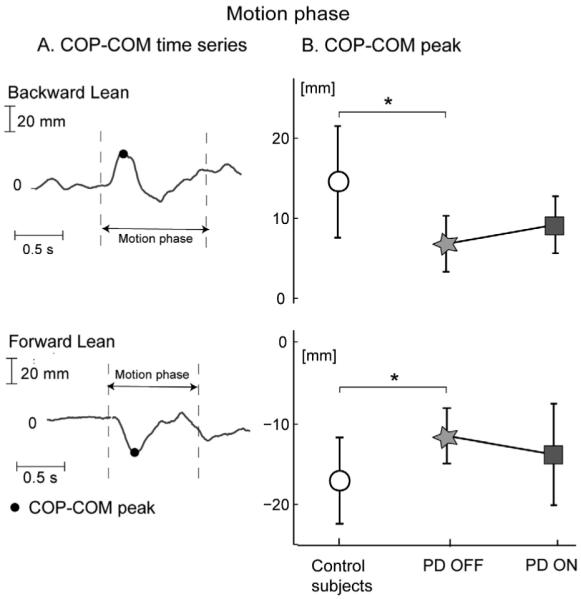
Findings: Functional limits of stability were significantly smaller in subjects with Parkinson's disease compared to control subjects. Subjects with Parkinson's disease maintained their stooped posture while leaning, initiated leaning with a smaller difference between center of pressure and center of mass and had a slower leaning velocity compared to control subjects. Levodopa enlarged the limits of stability in subjects with Parkinson's disease because of an increase in maximum forward, but not backward leans, but did not significantly improve postural alignment, preparation for a leaning movement, or velocity of leaning.
Interpretation: Parkinson's disease reduces functional limits of stability as well as the magnitude and velocity of postural preparation during voluntary, forward and backward leaning while standing. Levodopa improves the limits of stability but not the postural strategies used to achieve the leaning.
Figures
References
-
- Adkin AL, Bloem BR, Allum JH. Trunk sway measurements during stance and gait tasks in Parkinson’s disease. Gait Posture. 2005;22:240–249. - PubMed
-
- Bartolic A, Pirtosek Z, Rozman J, Ribaric S. Postural stability of Parkinson’s disease patients is improved by decreasing rigidity. Eur. J. Neurol. 2005;12:156–159. - PubMed
-
- Binda SM, Culham EG, Brouwer B. Balance, muscle strength, and fear of falling in older adults. Exp. Aging Res. 2003;29:205–219. - PubMed
-
- Blaszczyk JW, Klonowski W. Postural stability and fractal dynamics. Acta Neurobiol. Exp. (Wars) 2001;61:105–112. - PubMed
-
- Bloem BR, Beckley DJ, van Dijk JG. Are automatic postural responses in patients with Parkinson’s disease abnormal due to their stooped posture? Exp. Brain Res. 1999;124:481–488. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
