

Frequency of swing-segment stenosis in referred dialysis patients with angiographically documented lesions
- PMID: 18155537
- PMCID: PMC2692594
- DOI: 10.1053/j.ajkd.2007.09.012
Frequency of swing-segment stenosis in referred dialysis patients with angiographically documented lesions
Abstract
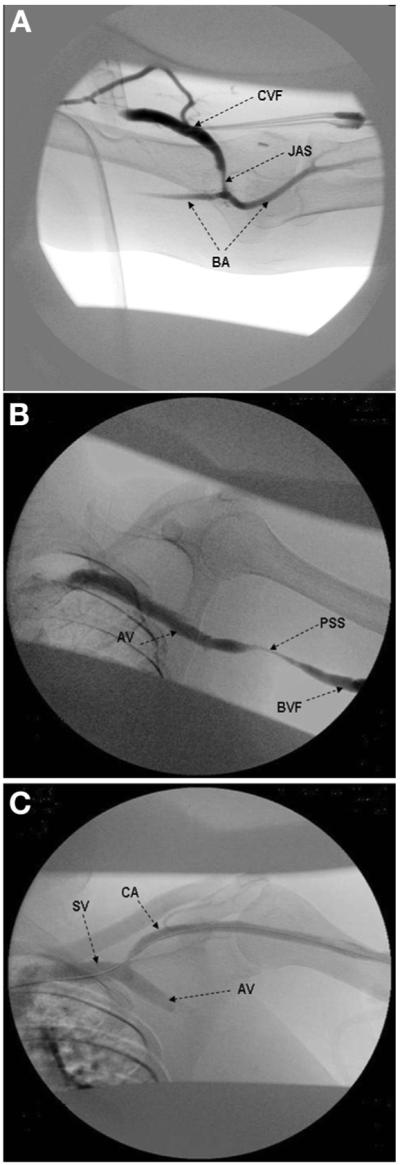
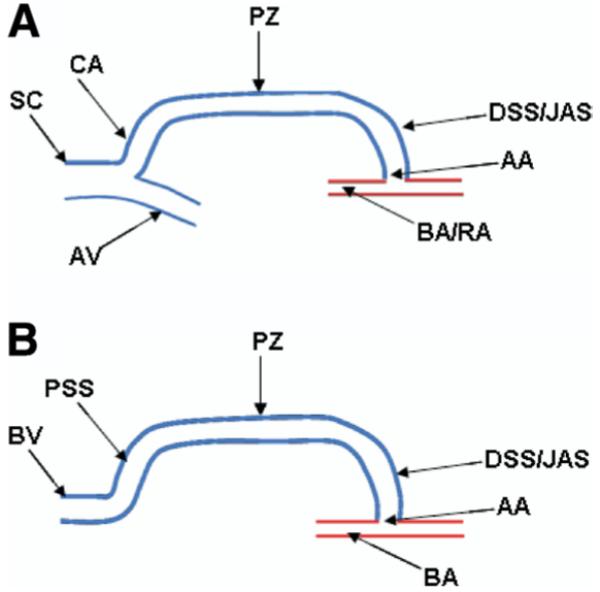
Background: The segment of the vein mobilized for arterial anastomosis in the creation of an arteriovenous fistula (AVF) is the swing segment. This segment may experience turbulent flow and altered shear mechanical stress that result in stenosis. We sought to determine the frequency of stenotic lesions in the swing segment.
Study design: Case series.
Settings & participants: From January 31, 2003, to June 30, 2005, records of all patients referred to an outpatient hemodialysis vascular access center for AVF dysfunction were reviewed (n = 484). Of these, 278 patients had angiographically documented stenosis (any degree of luminal narrowing) on their first visit.
Outcomes & measurements: Distribution of stenoses in different segments of the AVF. Swing-segment stenoses were classified as proximal (outflow into axillary vein system), distal or juxta-anastomotic (adjacent to the anastomosis), and the cephalic arch.
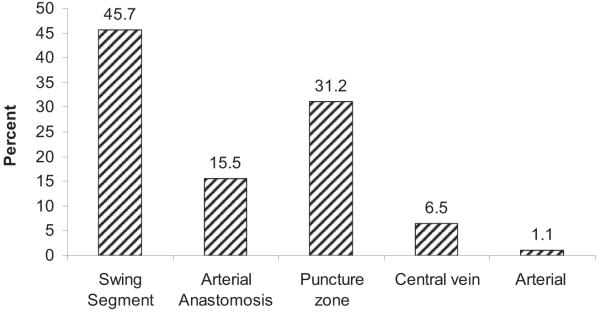
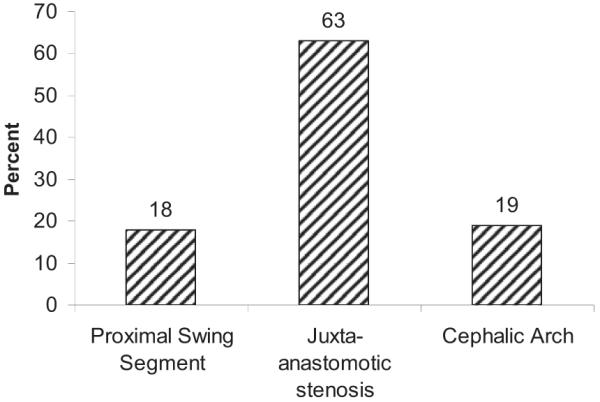
Results: Overall prevalence of angiographically documented swing segment stenosis (proximal, distal or juxta-anastomotic, and cephalic arch) was 45.7% (127 of 278 patients), whereas the remaining stenoses (151 of 278 patients) were distributed among the puncture zone, arterial, arterial anastomosis, and central veins. The most frequent location of the swing-segment stenosis was juxta-anatomosis (63%; 80 of 127 patients), followed by cephalic arch (19%; 24 of 127 patients) and proximal swing segment (18%; 23 of 127 patients). The distribution of swing-segment stenosis (n = 127) was equivalent among the various fistulas (brachial-cephalic, 35.4%; radial-cephalic, 33.9%; and brachial-basilic, 30.7%). Eighty-three percent of swing-segment stenoses were significant (>50% luminal narrowing) and underwent percutaneous transluminal angioplasty, with a 93% success rate.
Limitations: Retrospective nature of the study and potential selection bias.
Conclusion: In our population, swing-segment stenosis is the most common lesion in dysfunctional AVFs; juxta-anastomotic stenosis is the predominant lesion independent of fistula type. Whether the occurrence of swing-segment stenosis is caused by mobilization of the vein during surgery is not clear.
Figures
References
-
- National Kidney Foundation K/DOQI Clinical Practice Guidelines for Hemodialysis Adequacy: Update 2000. Am J Kidney Dis. 2001;37(suppl 1):S7–S64. - PubMed
-
- Ascher E, Gade P, Hingorani A, et al. Changes in the practice of angioaccess surgery: Impact of Dialysis Outcome and Quality Initiative recommendations. J Vasc Surg. 2000;31:84–92. - PubMed
-
- Gibson KD, Gillen DL, Caps MT, Kohler TR, Sherrard DJ, Stehman-Breen CO. Vascular access survival and incidence of revisions: A comparison of prosthetic grafts, simple autogenous fistulas, and venous transposition fistulas from the United States Renal Data System Dialysis Morbidity and Mortality Study. J Vasc Surg. 2001;34:694–700. - PubMed
-
- Beathard GA, Arnold P, Jackson J, Litchfield T. Aggressive treatment of early fistula failure. Kidney Int. 2003;64:1487–1494. - PubMed
-
- Grogan J, Castilla M, Lozanski L, Griffin A, Loth F, Bassiouny H. Frequency of critical stenosis in primary arteriovenous fistulae before hemodialysis access: Should duplex ultrasound surveillance be the standard of care? J Vasc Surg. 2005;41:1000–1006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
