

Improved contemporary surgical management of insulinomas: a 25-year experience at the Massachusetts General Hospital
- PMID: 18156937
- PMCID: PMC3806046
- DOI: 10.1097/SLA.0b013e31815792ed
Improved contemporary surgical management of insulinomas: a 25-year experience at the Massachusetts General Hospital
Abstract
Objective: To determine changes in the management strategy of patients with insulinomas and identify critical factors in patient outcome.
Background: Pancreatic insulinomas are rare neoplasms that are present in various ways. The optimal approach to localization, operative management, and follow-up of insulinomas is undetermined.
Methods: Sixty-one patients with a diagnosis of insulinoma requiring surgery at a tertiary care center between 1983 and 2007 were reviewed. Demographic details, mode of presentation, preoperative localization, operative procedures, and pathology data were assessed. The effect of different factors on survival was determined.
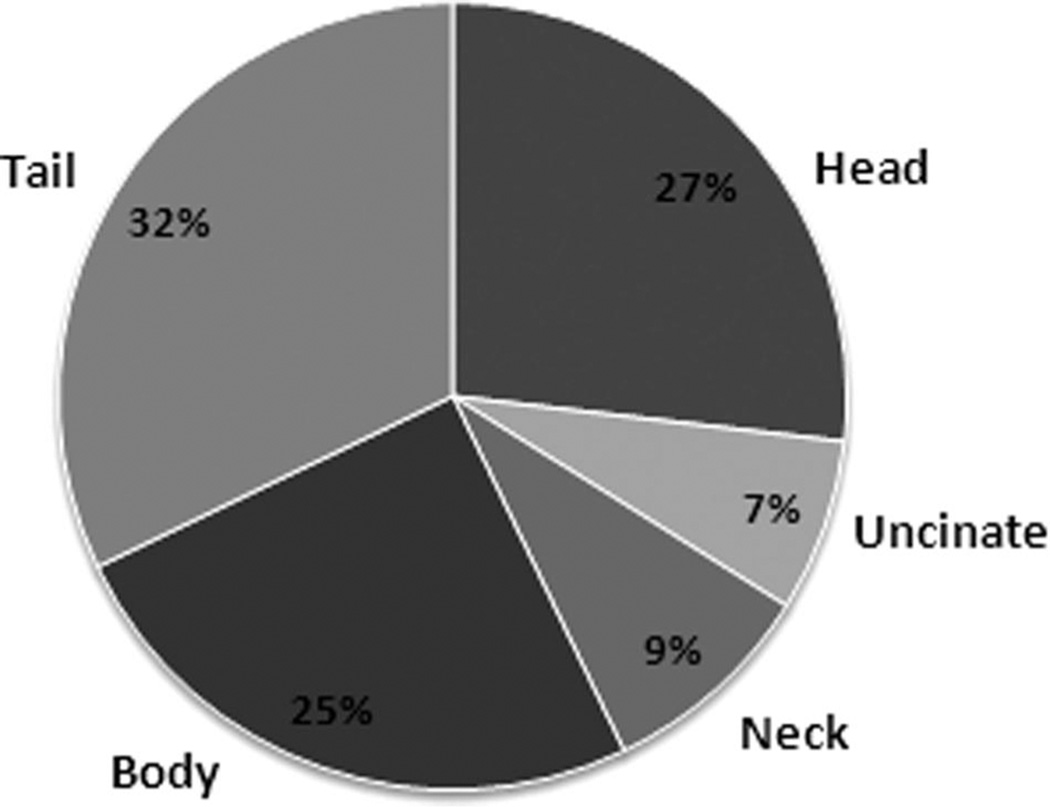
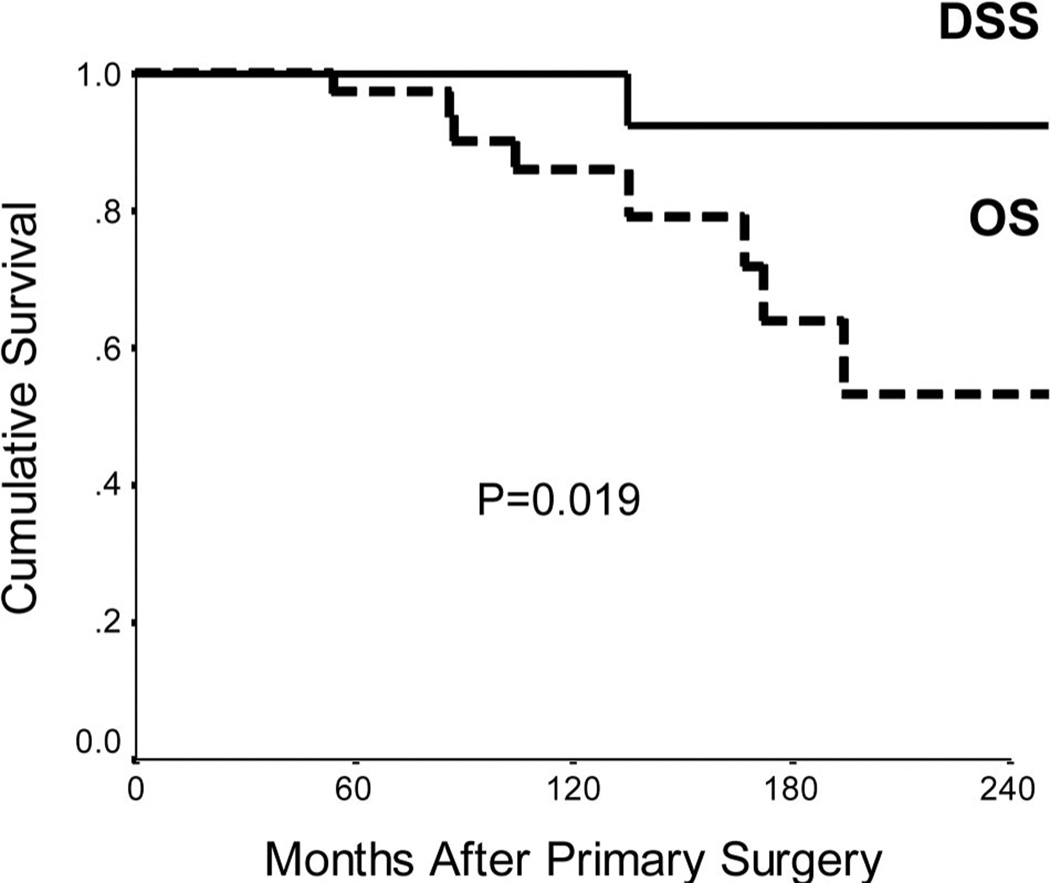
Results: Seven of 61 (11%) patients had a diagnosis of multiple endocrine neoplasia-type 1 (MEN-1). Multiple insulinomas were noted in 8% of cases and were more common in MEN-1 patients. The overall rate of malignancy was 8%. Confusion (67%), visual disturbances (42%), and diaphoresis (30%) were the most common presenting symptoms. Weight gain was noted in 44% of patients. The median duration of symptoms before diagnosis was 18 (1-240) months. The sensitivity of preoperative imaging of tumors before 1994 was 75%, compared with 98% after this period, which included use of endoscopic ultrasound scanning (P = 0.012). A combination of palpation and intraoperative ultrasound detected 92% of tumors. Distal pancreatectomy (40%), enucleation (34%), and pancreaticoduodenectomy (16%) were the most common procedures and pancreatic fistula occurred in 18% of patients. Three patients underwent noncurative distal pancreatectomy in the early period. The 10-year disease-specific and disease-free survival was 100% and 90% respectively. There were 5 patients with disease recurrence. Lymph node metastases (P < 0.001), lymphovascular invasion (P < 0.001), and the presence of MEN-1 (P = 0.035) were prognostically significant adverse factors in disease-free survival. Lymphovascular invasion was the only significant factor on multivariate analysis (P = 0.002).
Conclusion: Pancreatic insulinomas can be readily localized preoperatively with modern imaging to avoid unsuccessful blind pancreatic resection. Surgical resection is associated with low morbidity and mortality and achieves long-term disease-free survival in the absence of lymphovascular invasion.
Figures
References
-
- Service FJ, McMahon MM, O’Brien PC, et al. Functioning insulinomaincidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991;66:711–719. - PubMed
-
- Grant CS. Insulinoma. Best Pract Res Clin Gastroenterol. 2005;19:783–798. - PubMed
-
- Stefanini P, Carboni M, Patrassi N, et al. Beta-islet cell tumors of the pancreas: results of a study on 1,067 cases. Surgery. 1974;75:597–609. - PubMed
-
- Thakker RV. Multiple endocrine neoplasia type 1. Endocrinol Metab Clin North Am. 2000;29:541–567. - PubMed
-
- Mallery JS, Centeno BA, Hahn PF, et al. Pancreatic tissue sampling guided by EUS, CT/US, and surgery: a comparison of sensitivity and specificity. Gastrointest Endosc. 2002;56:218–224. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
