

Testosterone protects rat hearts against ischaemic insults by enhancing the effects of alpha(1)-adrenoceptor stimulation
- PMID: 18157169
- PMCID: PMC2259204
- DOI: 10.1038/sj.bjp.0707624
Testosterone protects rat hearts against ischaemic insults by enhancing the effects of alpha(1)-adrenoceptor stimulation
Abstract
Background and purpose: Testosterone alleviates symptoms in patients with ischaemic heart disease. Androgen receptors are present in the heart, and testosterone upregulates gene expression of cardiac beta(1)-adrenoceptors. We hypothesize that testosterone may confer cardioprotection by interacting with adrenoceptors.
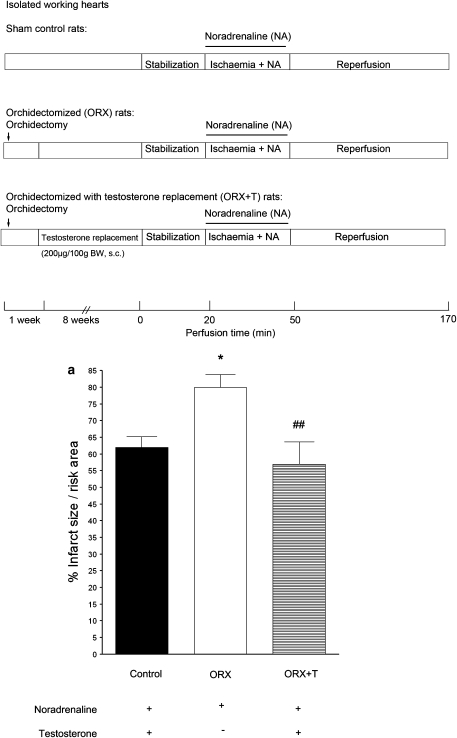
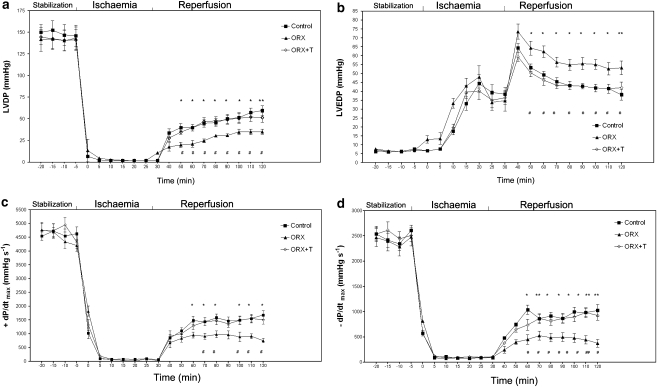
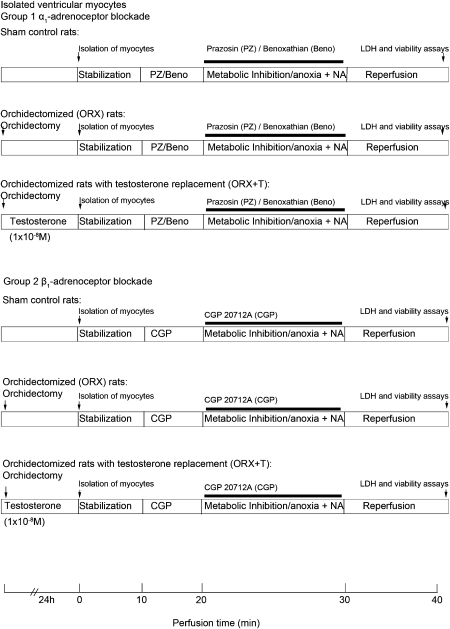
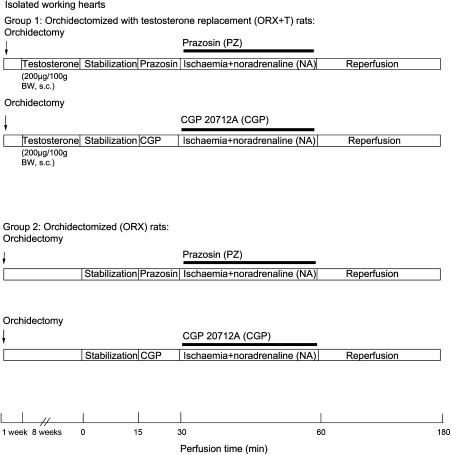
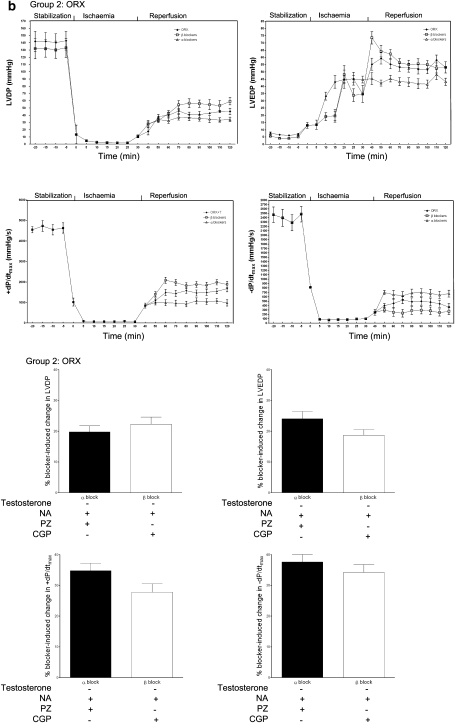
Experimental approach: In isolated perfused hearts and ventricular myocytes from orchidectomized rats without or with testosterone (200 microg/100 g) replacement, we first determined the effect of ischaemia/reperfusion in the presence of noradrenaline (10(-7) M). Then we determined the contribution of interactions between testosterone and alpha(1)- or beta(1)-adrenoceptors in cardiac injury/protection (infarct size, release of lactate dehydrogenase, viability of myocytes, recovery of contractile function and incidence of arrhythmias) upon ischaemia/reperfusion by pharmacological manipulation using selective adrenoceptor agonists (alpha(1)-adrenoceptor agonist: phenylephrine 10(-6) M; non-selective beta-adrenoceptor agonist: isoprenaline 10(-7) M) and antagonists (alpha(1): prazosin or benoxathian 10(-6) M; beta(1): CGP 20712A 5 x 10(-7) M). We also determined the expression of alpha(1) and beta(1)-adrenoceptor in the hearts from rats with and without testosterone.
Key results: Testosterone reduced injury induced by ischaemia/reperfusion and noradrenaline. This was achieved by enhancing the beneficial effect of alpha(1)-adrenoceptor stimulation, which was greater than the deleterious effect of beta(1)-adrenoceptor stimulation (also enhanced by testosterone). The effects of testosterone were abolished or attenuated by blockade of androgen receptors. Testosterone also enhanced the expression of alpha(1A) and beta(1)-adrenoceptor.
Conclusions and implications: Testosterone conferred cardioprotection by upregulating the cardiac alpha(1)-adrenoceptor and enhancing the effects of stimulation of this adrenoceptor. The effect of testosterone was at least partly mediated by androgen receptors.
Figures








Similar articles
-
Testosterone-augmented contractile responses to alpha1- and beta1-adrenoceptor stimulation are associated with increased activities of RyR, SERCA, and NCX in the heart.Am J Physiol Cell Physiol. 2009 Apr;296(4):C766-82. doi: 10.1152/ajpcell.00193.2008. Am J Physiol Cell Physiol. 2009. PMID: 19336623
-
Activation of alpha 1-adrenoceptors is not essential for the mediation of ischaemic preconditioning in rat heart.Clin Exp Pharmacol Physiol. 2002 Jan-Feb;29(1-2):11-7. doi: 10.1046/j.1440-1681.2002.03608.x. Clin Exp Pharmacol Physiol. 2002. PMID: 11906456
-
Exacerbation of reperfusion arrhythmias by alpha 1 adrenergic stimulation: a potential role for receptor mediated activation of sarcolemmal sodium-hydrogen exchange.Cardiovasc Res. 1995 Feb;29(2):222-30. Cardiovasc Res. 1995. PMID: 7736499
-
Pathophysiological relevance of the cardiac β2-adrenergic receptor and its potential as a therapeutic target to improve cardiac function.Eur J Pharmacol. 2013 Jan 5;698(1-3):39-47. doi: 10.1016/j.ejphar.2012.11.001. Epub 2012 Nov 23. Eur J Pharmacol. 2013. PMID: 23183106 Review.
-
Therapeutic potential of H(3)-receptor agonists in myocardial infarction.Expert Opin Investig Drugs. 2000 Nov;9(11):2537-42. doi: 10.1517/13543784.9.11.2537. Expert Opin Investig Drugs. 2000. PMID: 11060818 Review.
Cited by
-
Androgen Effects on the Adrenergic System of the Vascular, Airway, and Cardiac Myocytes and Their Relevance in Pathological Processes.Int J Endocrinol. 2020 Nov 12;2020:8849641. doi: 10.1155/2020/8849641. eCollection 2020. Int J Endocrinol. 2020. PMID: 33273918 Free PMC article. Review.
-
Clinical Significance of Serum Total Testosterone Concentration in Japanese Elderly Women With Pre-Heart Failure With Preserved Ejection Fraction.Cardiol Res. 2025 Jun 9;16(4):346-352. doi: 10.14740/cr2084. eCollection 2025 Aug. Cardiol Res. 2025. PMID: 40809732 Free PMC article.
-
Relationship of cardiac sympathetic nerve innervation and excitability to cardiac hypertrophy in very elderly male hypertensive patients.High Blood Press Cardiovasc Prev. 2013 Sep;20(3):115-21. doi: 10.1007/s40292-013-0018-z. Epub 2013 Aug 6. High Blood Press Cardiovasc Prev. 2013. PMID: 23918154
-
Testosterone Replacement Modulates Cardiac Metabolic Remodeling after Myocardial Infarction by Upregulating PPARα.PPAR Res. 2016;2016:4518754. doi: 10.1155/2016/4518754. Epub 2016 Jun 16. PPAR Res. 2016. PMID: 27413362 Free PMC article.
-
Improving translational research in sex-specific effects of comorbidities and risk factors in ischaemic heart disease and cardioprotection: position paper and recommendations of the ESC Working Group on Cellular Biology of the Heart.Cardiovasc Res. 2021 Jan 21;117(2):367-385. doi: 10.1093/cvr/cvaa155. Cardiovasc Res. 2021. PMID: 32484892 Free PMC article. Review.
References
-
- Banu KS, Govindarajulu P, Aruldhas MM. Testosterone and estradiol modulate TSH-binding in the thyrocytes of Wistar rats: influence of age and sex. J Steroid Biochem Mol Biol. 2001;78:329–342. - PubMed
-
- Callies F, Stromer H, Schwinger RH, Bolck B, Hu K, Frantz S, et al. Administration of testosterone is associated with a reduced susceptibility to myocardial ischemia. Endocrinology. 2003;144:4478–4483. - PubMed
-
- Communal C, Singh K, Pimentel DR, Colucci WS. Norepinephrine stimulates apoptosis in adult rat ventricular myocytes by activation of the β-adrenergic pathway. Circulation. 1998;98:1329–1334. - PubMed
-
- Communal C, Singh K, Sawyer DB, Colucci WS. Opposing effects of β1- and β2-adrenergic receptors on cardiac myocyte apoptosis: role of a pertussis toxin-sensitive G protein. Circulation. 1999;100:2210–2212. - PubMed
-
- Du XJ, Gao XM, Kiriazis H, Moore XL, Ming Z, Su Y, et al. Transgenic α1A-adrenergic activation limits post-infarct ventricular remodeling and dysfunction and improves survival. Cardiovasc Res. 2006;71:735–743. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
