

Toward early identification of acute lung injury in the emergency department
- PMID: 18163968
- PMCID: PMC2214900
- DOI: 10.2310/6650.2007.00026
Toward early identification of acute lung injury in the emergency department
Abstract
Background: There are no studies evaluating the epidemiology of pediatric acute lung injury (ALI) in the emergency department (ED), where early identification and interventions are most likely to be helpful. The purpose of this study was to describe the epidemiology of the ALI precursor acute hypoxemic respiratory failure (AHRF) in the ED.
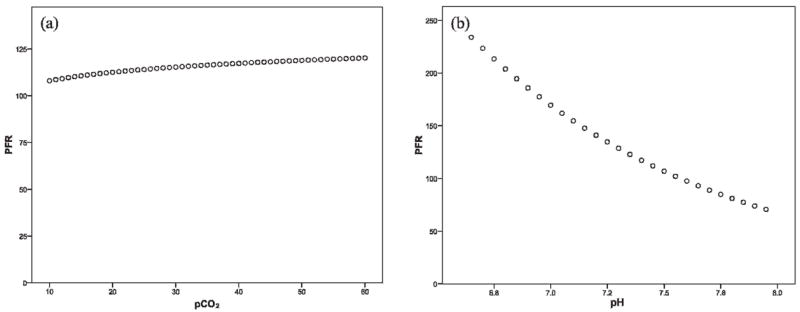
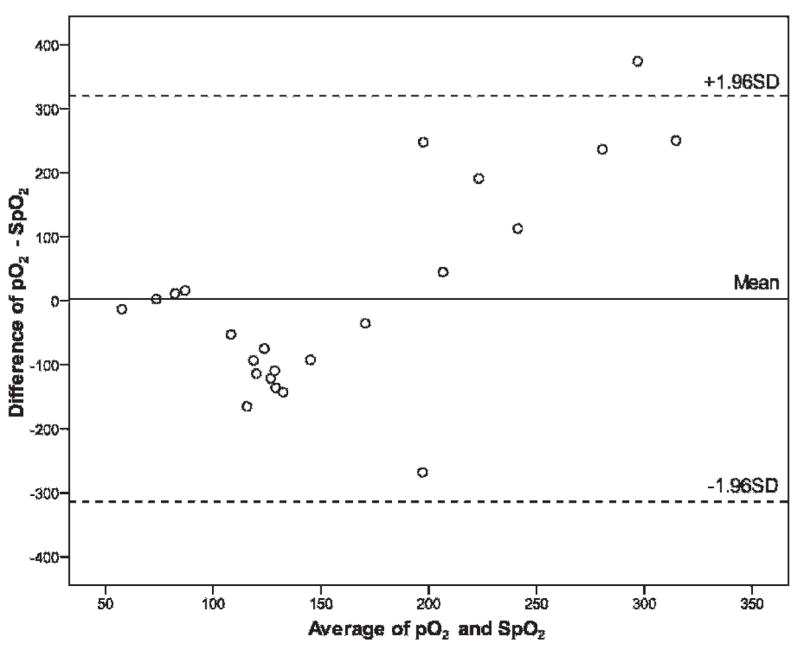
Methods: We analyzed 11,664 pediatric patient records from 16 EDs. Records were selected if oxygen saturation (SpO(2)) was recorded during the visit. Virtual partial pressure of oxygen (pO(2)) was calculated from SpO(2), thus allowing calculation of ratios of pO(2) to fraction of inspired oxygen (FiO(2)) (PFRs). Patients with a PFR < 300 were classified as having AHRF. Univariate analyses and logistic regression were used to test the association of clinical factors with the presence of AHRF and intubation.
Results: AHRF criteria (ie, PFR < 300) were met in 121 (2.9%) of the 4,184 patients with an oxygenation measurement. The following variables were independently associated with ALI: higher Pediatric Risk of Admission II score (adjusted odds ratio [95% confidence interval (CI)] = 1.12 [1.08-1.16]; p < .001), higher heart rate (1.02 [1.01-1.03]; p = .009), a positive chest radiograph (2.35 [1.02-5.43]; p = .045), and lower temperature (0.49 [0.36-0.68]; p < .001).The final model had an R(2) = .20.
Conclusion: We found nonintubated AHRF to be prevalent in the ED. The low R(2) for the regression model for AHRF underscores the lack of criteria for early identification of patients with respiratory compromise. Our findings represent an important first step toward establishing the true incidence of ALI in the pediatric ED.
Figures
Similar articles
-
A prospective cohort study of ALI/ARDS in the Tohoku district of Japan (second report).J Anesth. 2010 Jun;24(3):351-8. doi: 10.1007/s00540-010-0881-x. Epub 2010 Mar 27. J Anesth. 2010. PMID: 20349197
-
SpO2/FiO2 ratio on hospital admission is an indicator of early acute respiratory distress syndrome development among patients at risk.J Intensive Care Med. 2015 May;30(4):209-16. doi: 10.1177/0885066613516411. Epub 2013 Dec 20. J Intensive Care Med. 2015. PMID: 24362445
-
Prevalence of acute lung injury among medical patients in the emergency department.Acad Emerg Med. 2012 Sep;19(9):E1011-8. doi: 10.1111/j.1553-2712.2012.01429.x. Acad Emerg Med. 2012. PMID: 22978727
-
Epidemiology of acute lung injury.Crit Care Med. 2003 Apr;31(4 Suppl):S276-84. doi: 10.1097/01.CCM.0000057904.62683.2B. Crit Care Med. 2003. PMID: 12682453 Review.
-
Evolving epidemiology and definitions of the acute respiratory distress syndrome and early acute lung injury.Clin Chest Med. 2014 Dec;35(4):609-24. doi: 10.1016/j.ccm.2014.08.002. Epub 2014 Sep 26. Clin Chest Med. 2014. PMID: 25453413 Review.
Cited by
-
The utility of clinical predictors of acute lung injury: towards prevention and earlier recognition.Expert Rev Respir Med. 2010 Dec;4(6):785-97. doi: 10.1586/ers.10.78. Expert Rev Respir Med. 2010. PMID: 21128753 Free PMC article. Review.
-
Clinical review: Early treatment of acute lung injury--paradigm shift toward prevention and treatment prior to respiratory failure.Crit Care. 2012 Jun 19;16(3):223. doi: 10.1186/cc11144. Crit Care. 2012. PMID: 22713281 Free PMC article. Review.
-
Early acute lung injury: criteria for identifying lung injury prior to the need for positive pressure ventilation*.Crit Care Med. 2013 Aug;41(8):1929-37. doi: 10.1097/CCM.0b013e31828a3d99. Crit Care Med. 2013. PMID: 23782966 Free PMC article.
-
Identification of early acute lung injury at initial evaluation in an acute care setting prior to the onset of respiratory failure.Chest. 2009 Apr;135(4):936-943. doi: 10.1378/chest.08-2346. Epub 2009 Feb 2. Chest. 2009. PMID: 19188549 Free PMC article.
References
-
- Costil J, Cloup M, Leclerc F, et al. Acute respiratory distress syndrome (ARDS) in children: Multicenter Collaborative Study of the French Group of Pediatric Intensive Care. Pediatr Pulmonol Suppl. 1995;11:106–7. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. Report of the American-European Consensus Conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. The Consensus Committee Intensive Care Med. 1994;20:225–32. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. Report of the American-European Consensus Conference on acute respiratory distress syndrome: definitions, mechanisms, relevant outcomes, and clinical trial coordination. Consensus Committee J Crit Care. 1994;9:72–81. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149(3 Pt 1):818–24. - PubMed
-
- Huang DT, Angus DC. Designing clinical trials in acute lung injury/acute respiratory distress syndrome. Curr Opin Crit Care. 2006;12:32–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
