

Non-Hodgkin lymphoma and obesity: a pooled analysis from the InterLymph Consortium
- PMID: 18167059
- PMCID: PMC3928289
- DOI: 10.1002/ijc.23344
Non-Hodgkin lymphoma and obesity: a pooled analysis from the InterLymph Consortium
Abstract
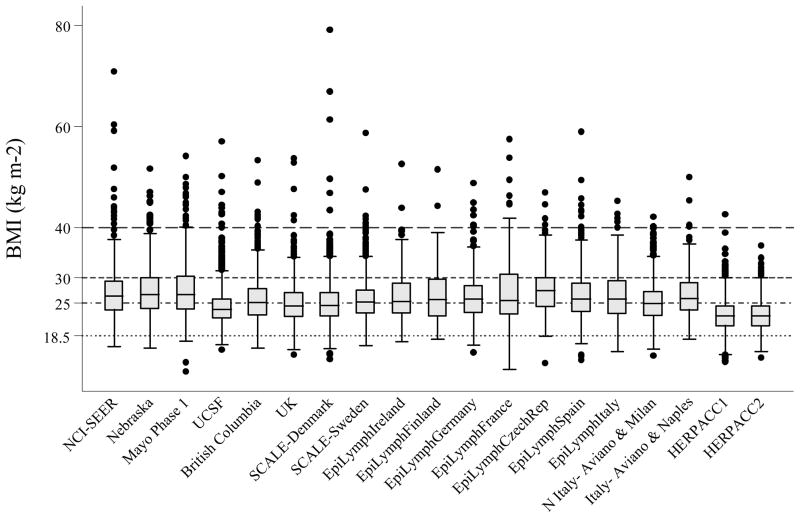
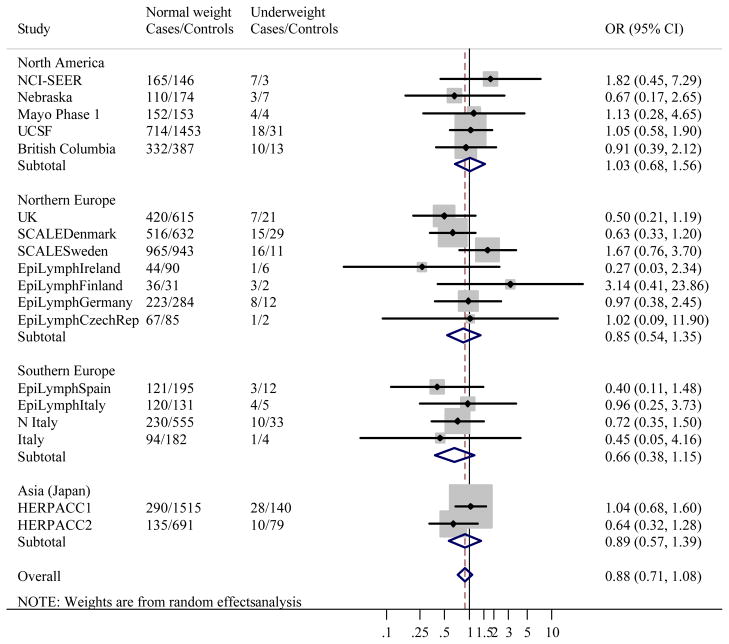
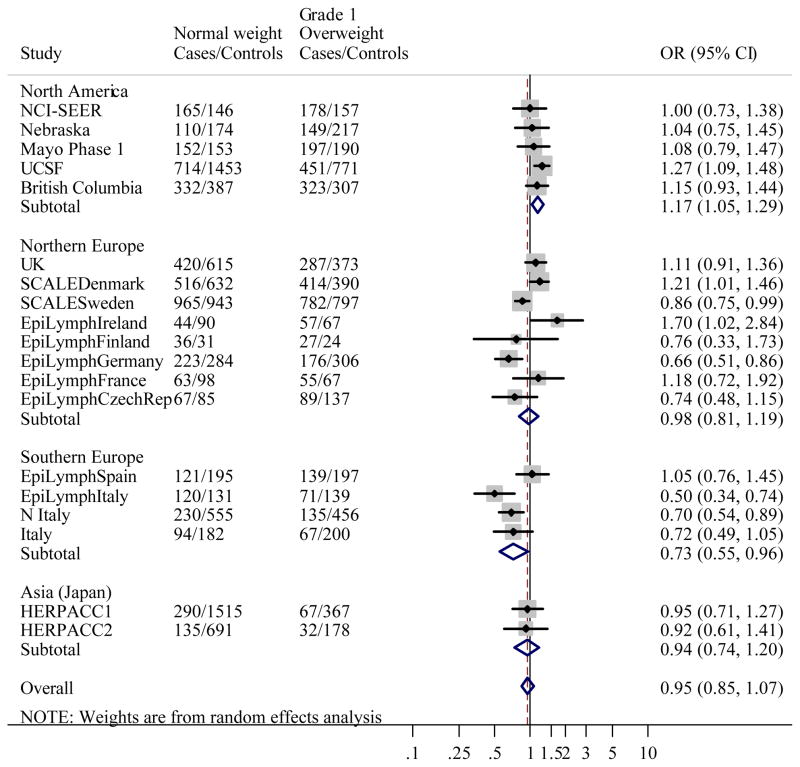
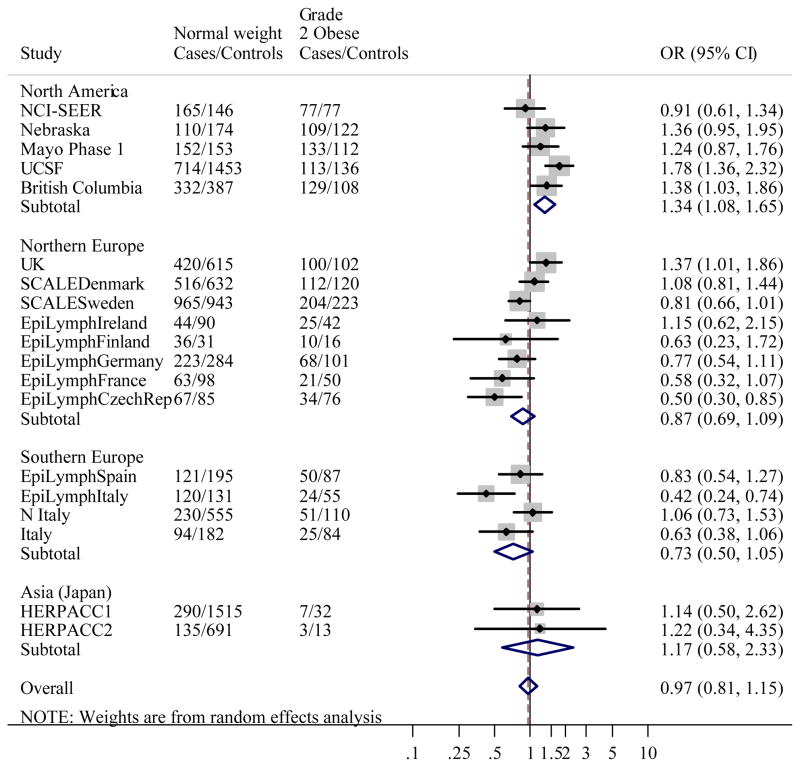
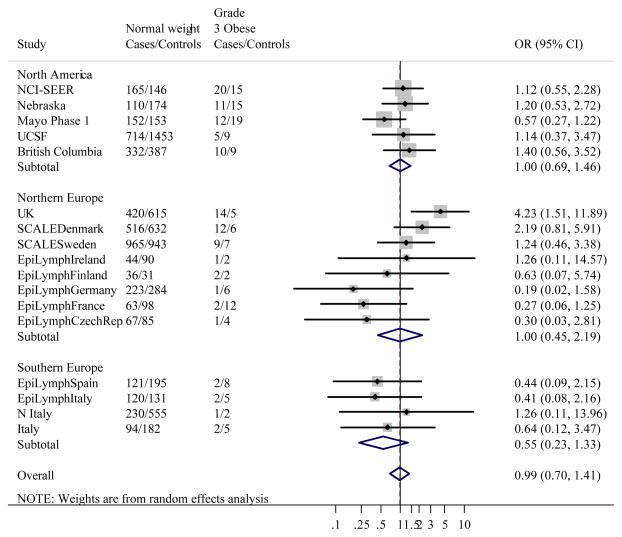
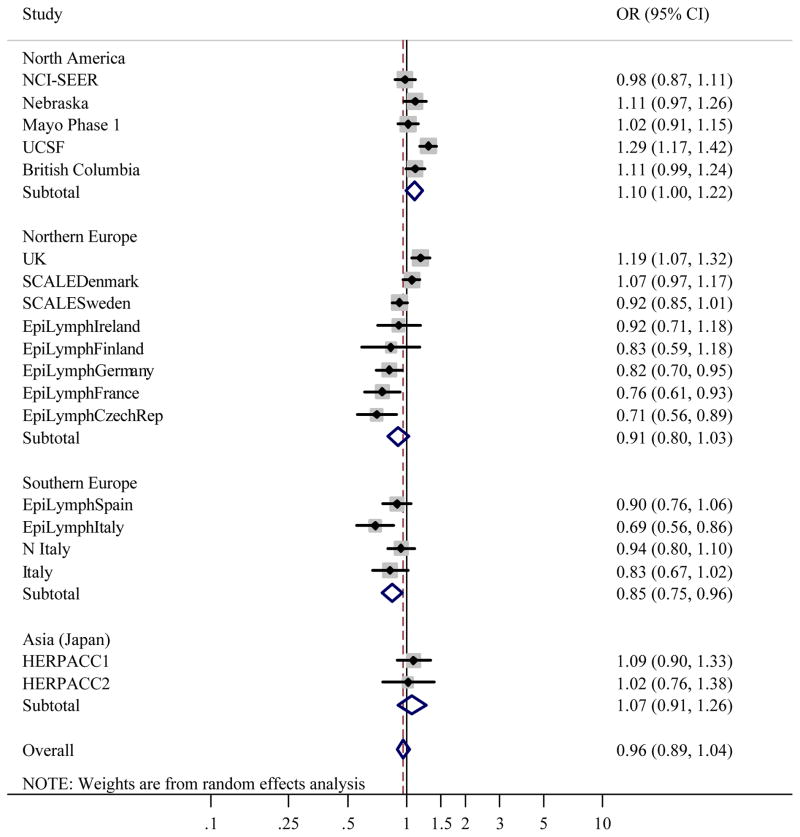
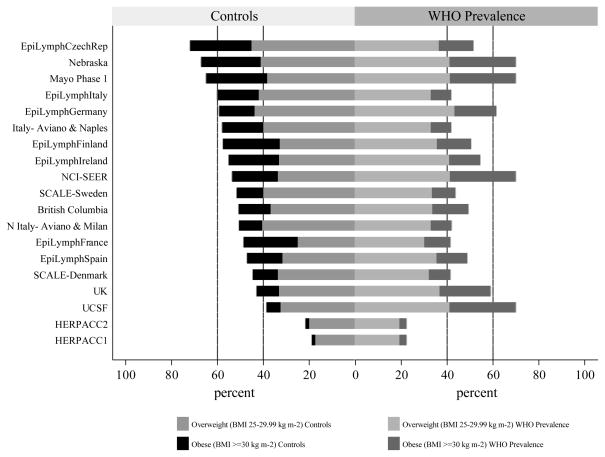
Nutritional status is known to alter immune function, a suspected risk factor for non-Hodgkin lymphoma (NHL). To investigate whether long-term over, or under, nutrition is associated with NHL, self-reported anthropometric data on weight and height from over 10,000 cases of NHL and 16,000 controls were pooled across 18 case-control studies identified through the International Lymphoma Epidemiology Consortium. Study-specific odds ratios (OR) were estimated using logistic regression and combined using a random-effects model. Severe obesity, defined as BMI of 40 kg m(-2) or more, was not associated with NHL overall (pooled OR = 1.00, 95% confidence interval (CI) 0.70-1.41) or the majority of NHL subtypes. An excess was however observed for diffuse large B-cell lymphoma (pooled OR = 1.80, 95% CI 1.24-2.62), although not all study-specific ORs were raised. Among the overweight (BMI 25-29.9 kg m(-2)) and obese (BMI 30-39.9 kg m(-2)), associations were elevated in some studies and decreased in others, while no association was observed among the underweight (BMI < 18.5 kg m(-2)). There was little suggestion of increasing ORs for NHL or its subtypes with every 5 kg m(-2) rise in BMI above 18.5 kg m(-2). BMI components height and weight were also examined, and the tallest men, but not women, were at marginally increased risk (pooled OR = 1.19, 95% CI 1.06-1.34). In summary, whilst we conclude that there is no evidence to support the hypothesis that obesity is a determinant of all types of NHL combined, the association between severe obesity and diffuse large B-cell lymphoma may warrant further investigation.
(c) 2007 Wiley-Liss, Inc.
Figures
Comment in
-
Obesity and the risk for non-Hodgkin lymphoma.Int J Cancer. 2008 Jul 15;123(2):490. doi: 10.1002/ijc.23523. Int J Cancer. 2008. PMID: 18449886 No abstract available.
References
-
- Marti A, Marcos A, Martinez JA. Obesity and immune function relationships. Obes Rev. 2001 May;2(2):131–40. - PubMed
-
- Samartin S, Chandra RK. Obesity, overnutrition and the immune system. Nutrition Research. 2001;21(1–2):243–62.
-
- Holly EA, Lele C, Bracci PM, McGrath MS. Case-control study of non-Hodgkin’s lymphoma among women and heterosexual men in the San Francisco Bay Area, California. Am J Epidemiol. 1999 Aug 15;150(4):375–89. - PubMed
-
- Wolk A, Gridley G, Svensson M, Nyren O, McLaughlin JK, Fraumeni JF, Adami HO. A prospective study of obesity and cancer risk (Sweden) Cancer Causes Control. 2001 Jan;12(1):13–21. - PubMed
-
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003 Apr 24;348(17):1625–38. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 PC067009/CN/NCI NIH HHS/United States
- N01 PC067010/PC/NCI NIH HHS/United States
- PC67009/PC/NCI NIH HHS/United States
- N01 PC067009/PC/NCI NIH HHS/United States
- CA50850/CA/NCI NIH HHS/United States
- N01 PC067008/PC/NCI NIH HHS/United States
- CA92153/CA/NCI NIH HHS/United States
- PC65064/PC/NCI NIH HHS/United States
- ZIA CP010170/ImNIH/Intramural NIH HHS/United States
- R01 CA051086/CA/NCI NIH HHS/United States
- R01 CA069269/CA/NCI NIH HHS/United States
- PC67008/PC/NCI NIH HHS/United States
- 5R01 CA69269-02/CA/NCI NIH HHS/United States
- PC71105/PC/NCI NIH HHS/United States
- N01 PC065064/PC/NCI NIH HHS/United States
- PC67010/PC/NCI NIH HHS/United States
- R01 CA092153/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
