

Understanding tumor endothelial cell abnormalities to develop ideal anti-angiogenic therapies
- PMID: 18167133
- PMCID: PMC11159852
- DOI: 10.1111/j.1349-7006.2007.00704.x
Understanding tumor endothelial cell abnormalities to develop ideal anti-angiogenic therapies
Abstract
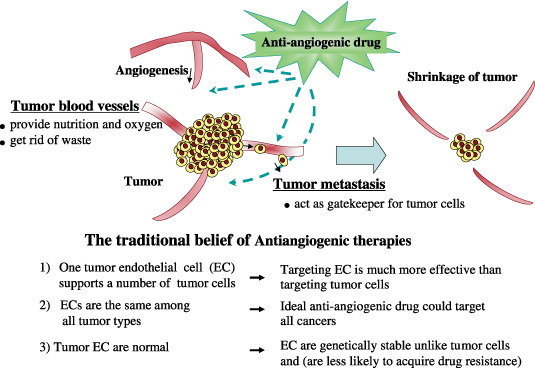
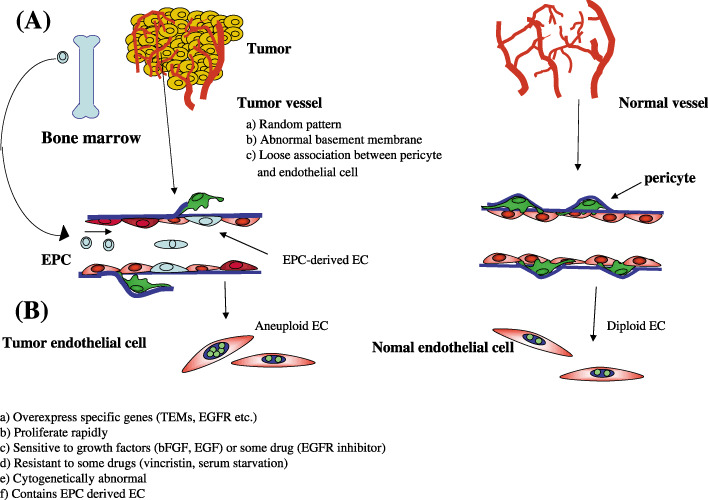
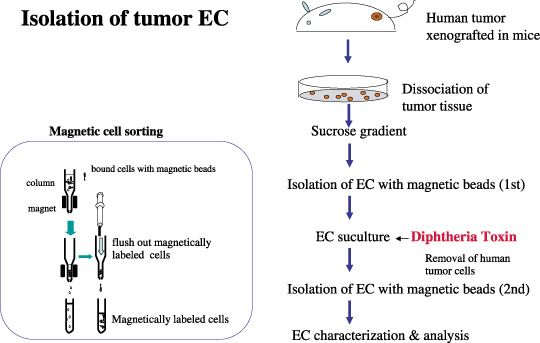
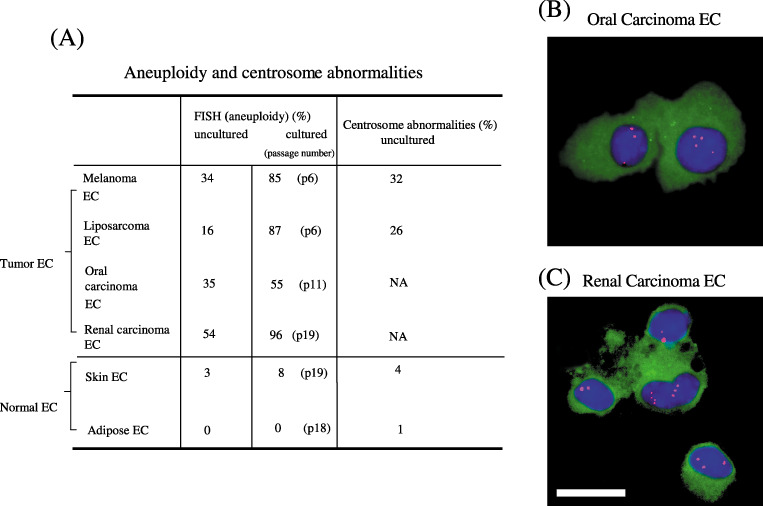
Tumor angiogenesis is necessary for solid tumor progression and metastasis. Tumor blood vessels have been shown to differ from their normal counterparts, for example, by changes in morphology. An important concept in tumor angiogenesis is that tumor endothelial cells are assumed to be genetically normal, even though these endothelial cells are structurally and functionally abnormal. To date, many anti-angiogenic drugs have been developed, but, their therapeutic efficacy is not dramatic and they have also been reported to cause toxic side effects. To develop ideal antiangiogenic therapies, understanding tumor endothelial cell abnormalities is important. We have isolated tumor endothelial cells from mouse tumor xenografts and have shown that tumor-associated endothelial cells are abnormal. Tumor-associated endothelial cells upregulate many genes, such as epidermal growth factor receptor (EGFR). Tumor-associated endothelial cells are also more sensitive to EGF. They also have relatively large, heterogeneous nuclei. Unexpectedly, tumor endothelial cells are cytogenetically abnormal. Fluorescence in situ hybridization (FISH) analysis showed that freshly isolated uncultured tumor endothelial cells were aneuploid and had abnormal multiple centrosomes. The degree of aneuploidy was exacerbated by passage in culture. In marked contrast, freshly isolated normal skin and adipose endothelial cells were diploid. They had normal centrosomes and remained cytogenetically stable in culture even up to 20 passages. We conclude that tumor endothelial cells can acquire cytogenetic abnormalities while in the tumor microenvironment. Questions as to whether or not tumor endothelial cells become resistant to antiangiogenic drugs are thus raised. Our preliminary data show that tumor endothelial cells are more resistant to certain chemotherapeutic drugs. Studies to evaluate the mechanism for cytogenetic abnormalities in tumor endothelial cells are underway. It is becoming quite clear that the tumor vasculature is much more complex and unpredictable than initially perceived. Here, we provide an overview of the current studies on tumor endothelial cell abnormalities.
Figures
References
-
- Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med 1971; 285: 1182–6. - PubMed
-
- Folkman J, Kerbel R. Role of angiogenesis in tumor growth and metastasis Clinical translation of angiogenesis inhibitors. Semin Oncol 2002; 29: 15–18. - PubMed
-
- Folkman J. Angiogenesis: an organizing principle for drug discovery? Nat Rev Drug Discov 2007; 6: 273–86. - PubMed
-
- Johnson DH, Fehrenbacher L, Novotny WF et al . Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non‐small‐cell lung cancer. J Clin Oncol 2004; 22: 2184–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
