

Estimating the rate of progressive visual field damage in those with open-angle glaucoma, from cross-sectional data
- PMID: 18172076
- PMCID: PMC2246309
- DOI: 10.1167/iovs.07-0866
Estimating the rate of progressive visual field damage in those with open-angle glaucoma, from cross-sectional data
Abstract
Purpose: To estimate the rate of visual field progression in open-angle glaucoma (OAG) subjects, by using data from population-based cross-sectional studies.
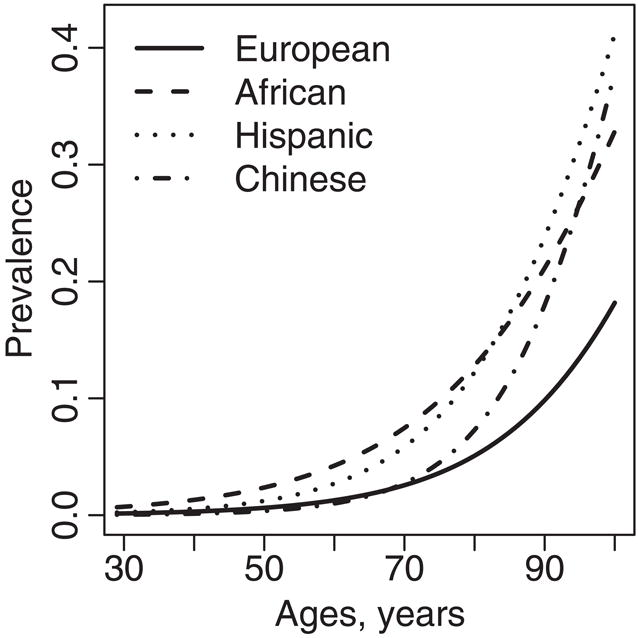
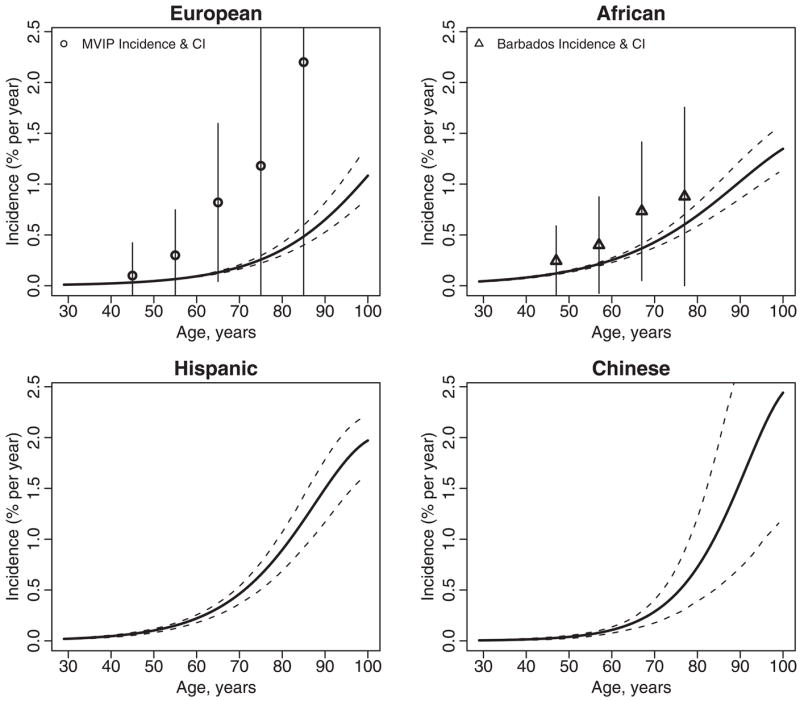
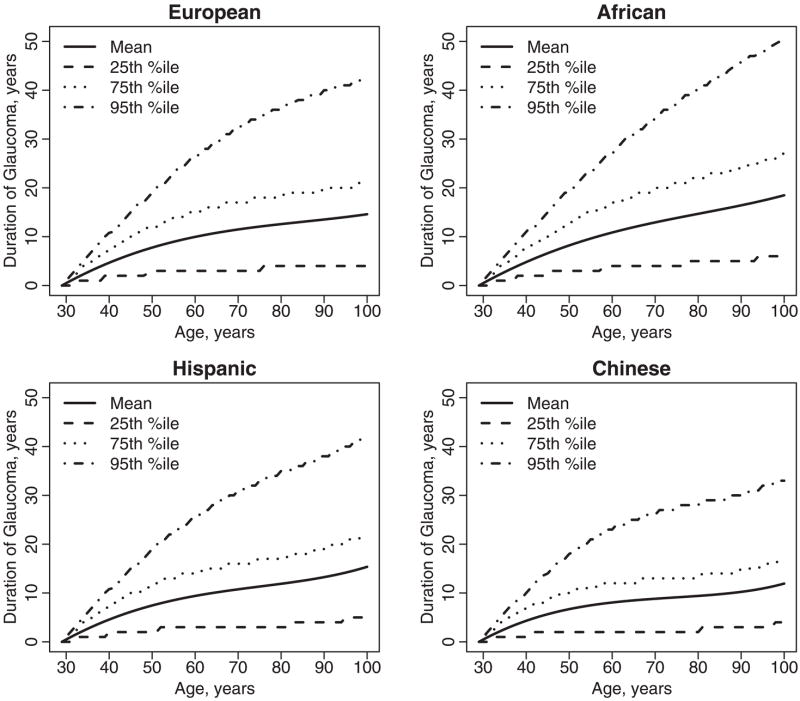
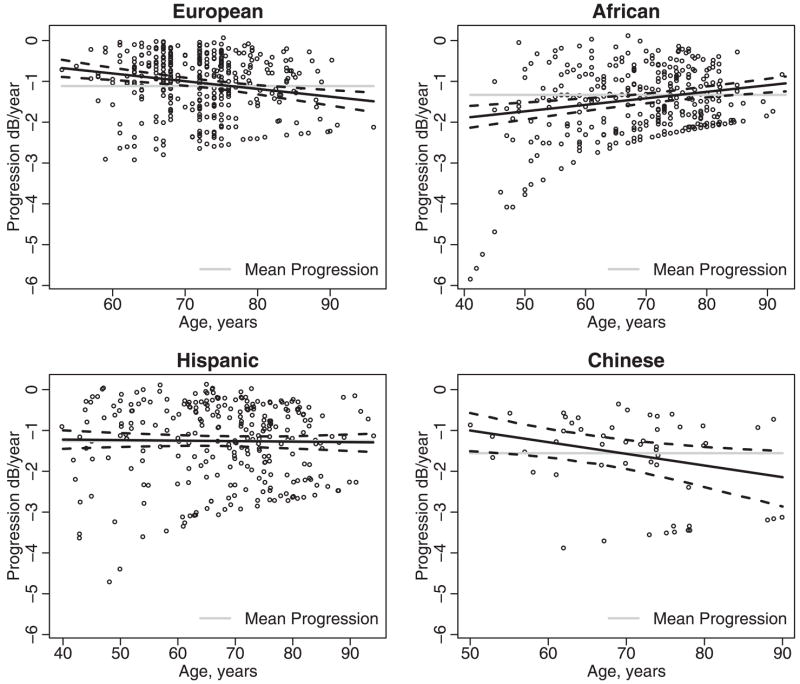
Methods: Subjects with OAG were identified in nine surveys of randomly sampled populations using standard criteria for glaucomatous optic neuropathy. Subjects were of European, African, Chinese, and Hispanic ethnicity. The measure of OAG damage was the mean deviation (MD) of an automated visual field test (Humphrey Field Analyzer; Carl Zeiss Meditec, Inc., Dublin, CA). The rate of progression was the mean of all subjects' damage in the worse eye divided by an average time since onset. Time since onset was estimated from age-specific prevalence rates.
Results: A total of 1066 subjects with OAG contributed visual field data. The mean worsening in decibels per year was: European-derived, -1.12; Hispanic, -1.26; African-derived, -1.33; and Chinese -1.56 (difference among ethnicities, P = 0.16). The mean duration of disease was lowest among Chinese persons at 10.5 years (95% CI: 8.8-12.6) and was highest in African-derived subjects at 15.4 years (95% CI: 14.6-15.9). The progression rate was not consistently related to age or gender. By combining disease duration and progression rate, the model predicted that 15% or fewer of the worse eyes would reach the end of the field damage scale in the patient's lifetime.
Conclusions: The estimates of typical worsening per year in the worse eye among subjects with OAG suggested slightly more rapid progression than in some clinic-based studies. The rate did not differ significantly by ethnicity or gender, but was worse in those with known, treated OAG and in pseudophakic subjects.
Figures
References
-
- Ellwein LB, Urato CJ. Use of eye care and associated charges among the Medicare population: 1991–1998. Arch Ophthalmol. 2002;120:804–811. - PubMed
-
- Schappert SM. Office visits for glaucoma: United States, 1991–92; advance data from vital and health statistics. Hyattsville, MD: National Center for Health Statistics; 1995. p. 262. - PubMed
-
- Fiscella RG, Green A, Patuszynski DH, Wilensky J. Medical therapy cost considerations for glaucoma. Am J Ophthalmol. 2003;136:18–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
