

A single posterior approach for multilevel modified vertebral column resection in adults with severe rigid congenital kyphoscoliosis: a retrospective study of 13 cases
- PMID: 18172699
- PMCID: PMC2270391
- DOI: 10.1007/s00586-007-0566-9
A single posterior approach for multilevel modified vertebral column resection in adults with severe rigid congenital kyphoscoliosis: a retrospective study of 13 cases
Abstract
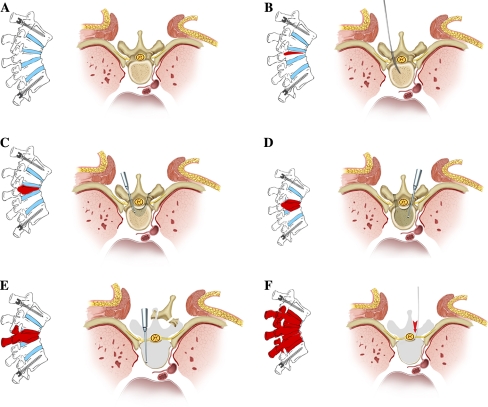
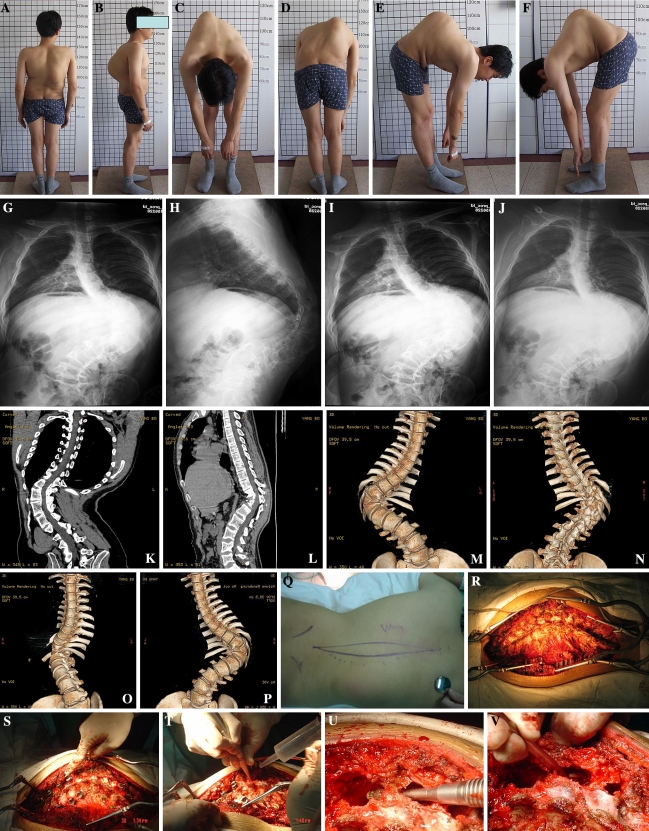
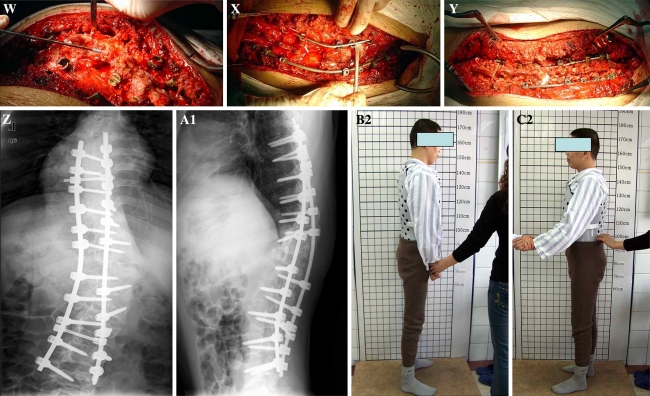
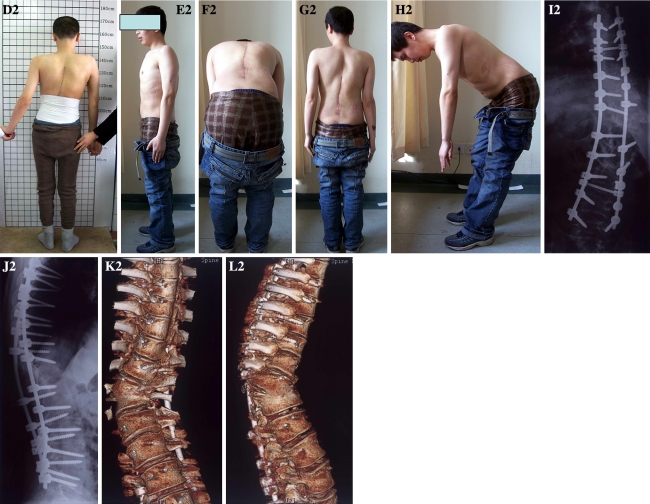
We report a multilevel modified vertebral column resection (MVCR) through a single posterior approach and clinical outcomes for treatment of severe congenital rigid kyphoscoliosis in adults. Transpedicular eggshell osteotomies and vertebral column resection are two techniques for the surgical treatment of rigid severe spine deformities. The authors developed a new technique combining the two surgical methods as a MVCR, through a single posterior approach, for surgical treatment of severe congenital rigid kyphoscoliosis in adults. Thirteen adult patients with severe rigid congenital kyphoscoliosis deformity were treated by a single posterior approach using a MVCR technique. The surgery processes included a one-stage posterior transpedicular eggshell technique first, and then expanded the eggshell technique to adjacent intervertebra space through abrasive reduction of the vertebral cortices from inside out. All posterior vertebral elements were removed including the cortical vertebral bone around the neural canal. Range of resection of the vertebral column at the apex of the deformity included apical vertebra and both cephalic and/or caudal adjacent wedged vertebrae. Totally, 32 vertebrae had been removed in 13 patients, with 2.42 vertebrae being removed on average in each case. The average fusion extent was 7.69 vertebrae. Mean operation time was 266 min with average blood loss of 2,411.54 ml during operation. Patients were followed up for an average duration of 2.54 years. Deformity correction was 59% in the coronal plane (from 79.7 degrees to 32.4 degrees ) postoperatively and 33.7 degrees (57% correction) at 2 years follow-up. In the sagittal plane, correction was from preoperative 85.9 degrees to 27.5 degrees immediately after operation, and 32.0 degrees at 2 years follow-up. Postoperative pain was reduced from preoperative 1.77 to 0.54 at 2 years follow-up in visual analog scale. SRS-24 scale was from 38.2 preoperatively to 76.9 at 2 years follow-up postoperative. Complications were encountered in four patients (30.7%) with transient neurology that spontaneously improved without further treatment within 3 months. MVCR technique through a single posterior approach is an effective procedure for the surgical treatment of severe congenital rigid kyphoscoliosis in adults.
Figures

References
-
- Baba H, Maezawa Y, Kamitani K, et al. Osteoporotic vertebral collapse with late neurological complications. Paraplegia. 1995;33:281–289. - PubMed
-
- Bradford DS, Boachie-Adjei O. One-stage anterior and posterior hemivertebral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am. 1990;72:536–540. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
