

Electrophysiological characteristics of fetal atrioventricular block
- PMID: 18174041
- PMCID: PMC3296565
- DOI: 10.1016/j.jacc.2007.06.060
Electrophysiological characteristics of fetal atrioventricular block
Abstract
Objectives: The purpose of our work was to define the complex electrophysiological characteristics seen in second- (2 degrees) and third-degree (3 degrees) atrioventricular block (AVB) and to longitudinally follow the development of atrial and ventricular heart rate and rhythm patterns with a goal of identifying heart rate and rhythm patterns associated with urgent delivery or neonatal pacing.
Background: The electrophysiological characteristics of congenital AVB before birth have not been extensively studied, yet the mortality from this disease is substantial. Along with advances in fetal therapies and interventions, a comprehensive natural history specific to the etiology of AVB, as well as the electrophysiological factors influencing outcome, are needed to best select treatment options.
Methods: Twenty-eight fetuses with AVB were evaluated by fetal magnetocardiography; 21 fetuses were evaluated serially.
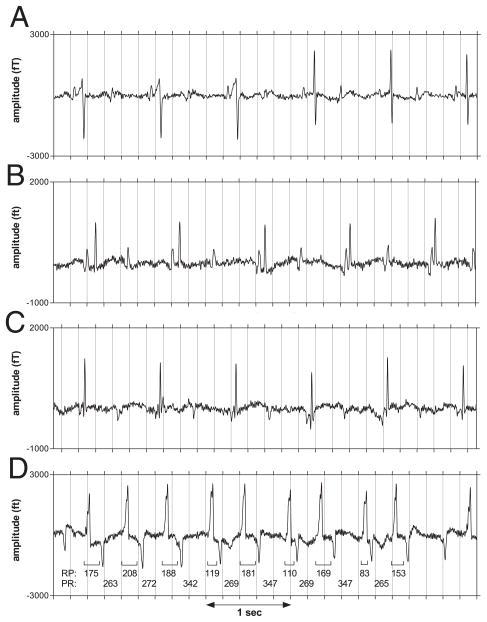
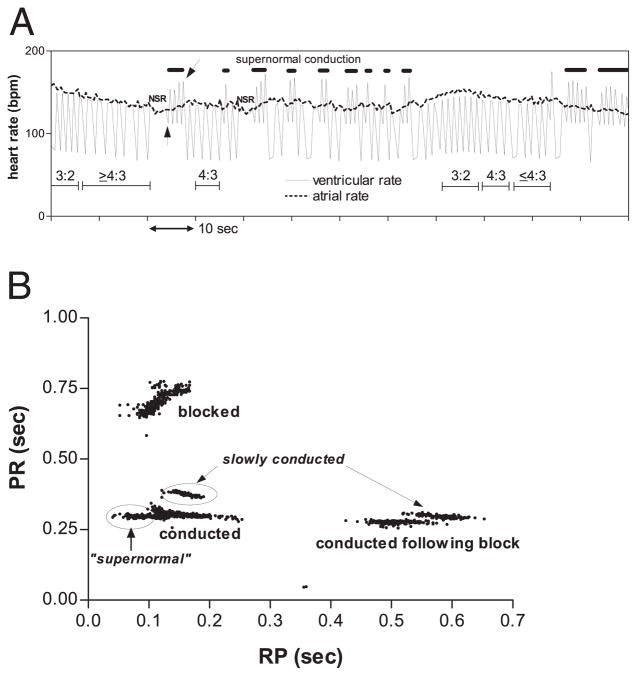
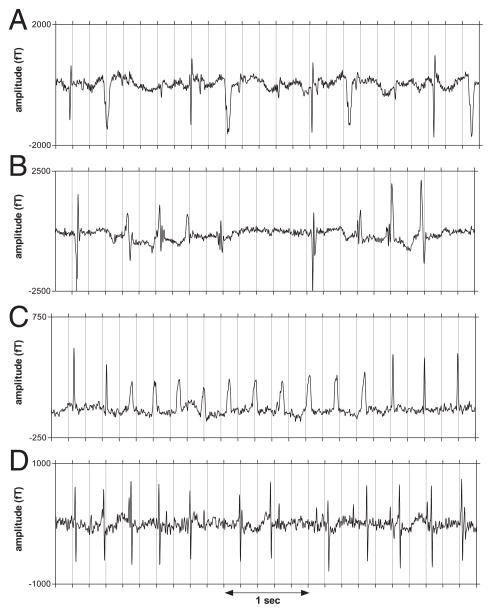
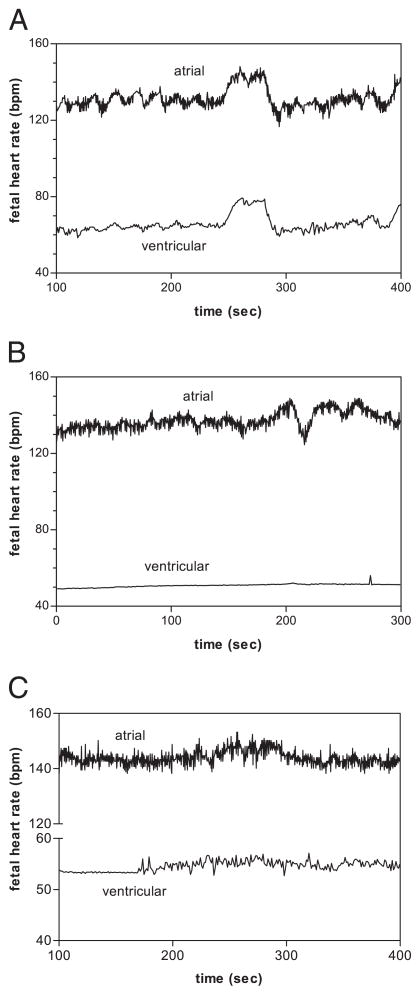
Results: Fetuses with 2 degrees AVB and isolated 3 degrees AVB showed: 1) diverse atrial rhythms and mechanisms of atrioventricular conduction during 2 degrees AVB; 2) junctional ectopic tachycardia and ventricular tachycardia during 3 degrees AVB; 3) reactive ventricular and atrial fetal heart rate (FHR) tracings at ventricular rates >56 beats/min; and 4) flat ventricular FHR tracings at ventricular rates <56 beats/min despite reactive atrial FHR tracings. In contrast, fetuses with 3 degrees AVB associated with structural cardiac disease exhibited predominantly nonreactive heart rate tracings and simpler rhythms.
Conclusions: Second-degree AVB, isolated 3 degrees AVB, and 3 degrees AVB associated with structural cardiac disease manifest distinctly different electrophysiological characteristics and outcome. Fetuses with 2 degrees AVB or isolated 3 degrees AVB commonly exhibited complex, changing heart rate and rhythm patterns; all 19 delivered fetuses are alive and healthy. Fetuses with structural cardiac disease and 3 degrees AVB exhibited largely monotonous heart rate and rhythm patterns and poor prognosis. Junctional ectopic tachycardia and/or ventricular tachycardia may be characteristic of an acute stage of heart block.
Figures
Comment in
-
New insights into fetal atrioventricular block using fetal magnetocardiography.J Am Coll Cardiol. 2008 Jan 1;51(1):85-6. doi: 10.1016/j.jacc.2007.09.016. J Am Coll Cardiol. 2008. PMID: 18174042 No abstract available.
References
-
- Menendez T, Achenbach S, Beinder E, et al. Usefulness of magnetocardiography for the investigation of fetal arrhythmias. Am J Cardiol. 2001;88:334–6. - PubMed
-
- Van Leeuwen P, Hailer B, Bader W, Geissler J, Trowitzsch E, Gronemeyer D. Magnetocardiography in the diagnosis of fetal arrhythmia. Br J Obstet Gynaecol. 1999;11:1200–8. - PubMed
-
- Wakai RT, Leuthold AC, Cripe L, Martin CB. Assessment of fetal rhythm in complete congenital heart block by magnetocardiography. Pacing Clin Electrophysiol. 2000;23:1047–50. - PubMed
-
- Zhao H, Wakai RT. Simultaneity of foetal heart rate acceleration and foetal trunk movement determined by foetal magnetocardiogram actocardiography. Phys Med Biol. 2002;47:839–46. - PubMed
-
- Leuthold A, Wakai RT, Martin CB. Noninvasive in utero assessment of PR and QRS intervals from the fetal magnetocardiogram. Early Hum Dev. 1999;54:235–43. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
