

Review
doi: 10.1007/s00401-007-0320-8.
Epub 2008 Jan 4.
Diagnosis of inflammatory demyelination in biopsy specimens: a practical approach
Affiliations
- PMID: 18175128
- PMCID: PMC2668559
- DOI: 10.1007/s00401-007-0320-8
Item in Clipboard
Review
Diagnosis of inflammatory demyelination in biopsy specimens: a practical approach
Acta Neuropathol.
2008 Mar.
Abstract
Multiple sclerosis is the most frequent demyelinating disease in adults. It is characterized by demyelination, inflammation, gliosis and a variable loss of axons. Clinically and histologically, it shares features with other demyelinating and/or inflammatory CNS diseases. Diagnosis of an inflammatory demyelinating disease can be challenging, especially in small biopsy specimens. Here, we summarize the histological hallmarks and most important neuropathological differential diagnoses of early MS, and provide practical guidelines for the diagnosis of inflammatory demyelinating diseases.
Figures
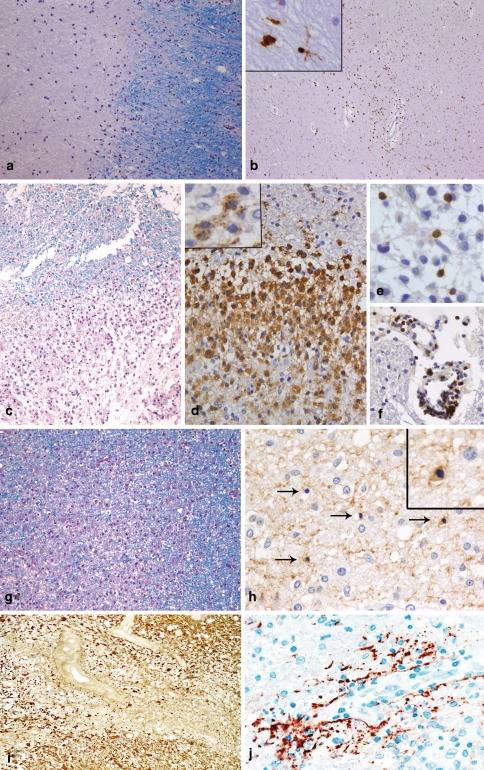
Chronic and early MS lesions. Chronic MS lesions have a sharp border with the surrounding normal appearing white matter [NAWM; LFB-PAS staining; (a)]. Frequently, the demyelinated lesion centre is hypocellular while the lesion border and the normal appearing white matter show an increased number of macrophages and/or microglia (immunohistochemistry for the macrophage/microglial marker KiM1P (b) and insert). Early MS lesions with pattern I are characterized by a sharp border with the NAWM [LFB-PAS staining; (c)]. The inflammatory infiltrates are dominated by foamy macrophages [immunohistochemistry for KiM1P (d)], which may contain myelin degradation products in their cytoplasm (immunohistochemistry for the myelin protein MBP (insert in d)). T cells are diffusely distributed within the parenchyma of the lesion (e), but may also be found perivascularly in NAWM [immunohistochemistry for CD3; (f)]. Pattern III lesions show an ill-defined lesion border [LFB-PAS staining; (g)]. In areas of active demyelination and NAWM, numerous dying oligodendrocytes (arrows) with condensed nuclei are observed [immunohistochemistry for CNP; (h)]. The insert in h shows a higher magnification of a CNP-positive oligodendrocyte with a condensed nucleus. In NMO, a loss of astrocytes and glial fibres [immunohistochemistry for GFAP; (i)] as well as a perivascular deposition of complement is observed [immunohistochemistry for C9neo; (j)]
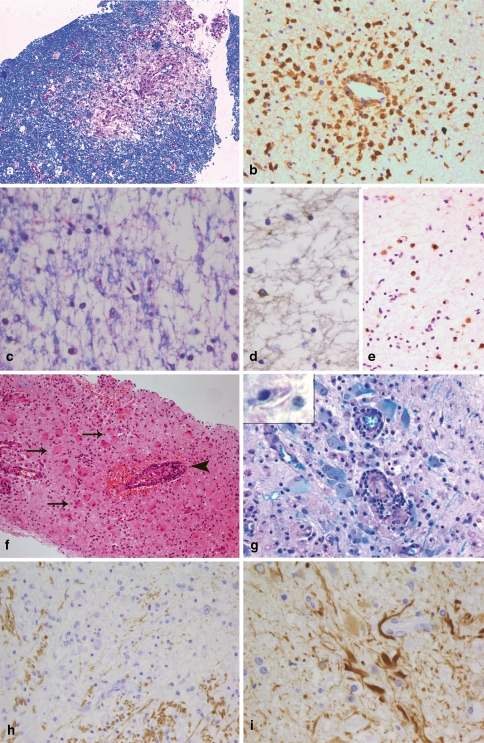
Different demyelinating diseases. ADEM is characterized by very limited perivascular demyelination [LFB-PAS; (a)] and perivascular infiltrates that consist mostly of foamy macrophages [immunohistochemistry for KiM1P; (b)]. In vanishing white matter, a diffuse loss of myelin is observed [LFB-PAS; (c)]. The number of oligodendrocytes in affected white matter areas is markedly reduced [immunohistochemistry for CNPase (d)]. In contrast to early MS lesions, the demyelinated lesions are infiltrated by relatively few macrophages [immunohistochemistry for KiM1P; (e)]. In X-linked adrenoleukodystrophy, numerous bizarre astrocytes can be found within the lesions (arrows in f) as well as lymphocytic perivascular infiltrates (arrowhead in f; haematoxylin and eosin staining). The lesion areas are completely demyelinated (g) and in macrophages needle-like inclusions may be found (insert in g). In Alexander’s disease large CNS areas with an almost complete loss of myelin are found [immunohistochemistry for MBP; (h)]. The histopathological characteristic of Alexander’s disease is numerous GFAP-positive Rosenthal fibres [immunohistochemistry for GFAP; (i)]
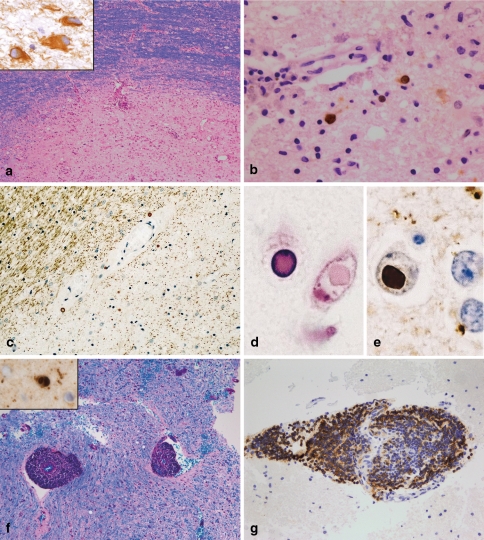
PML, SSPE and viral encephalitis. PML lesions may be characterized by a sharp lesion border [LFB-PAS; (a)]. The histopathological hallmarks are bizarre astrocytes (immunohistochemistry for GFAP; insert in a) and viral inclusion bodies in oligodendrocytes and astrocytes [immunohistochemistry with antibodies recognizing JC antigens; (b)]. SSPE is characterized by demyelinated lesions often accompanied by extensive axonal loss [immunohistochemistry for MAG; (c)]. In oligodendroglial nuclei, viral inclusions can be found, which are intensively eosinophilic [haematoxylin and eosin; (d)]. Measles virus antigen can be identified by immunohistochemistry (e). In acute viral encephalitis, e.g. in acute measles encephalitis, marked perivascular infiltrates are observed while the myelin is not affected [LFB-PAS staining; (f)]. In this patient, measles virus antigen could be detected in oligodendroglial nuclei (insert in f). The perivascular infiltrates may be dominated by B cells [immunohistochemistry for the B cell marker CD20; (g)]
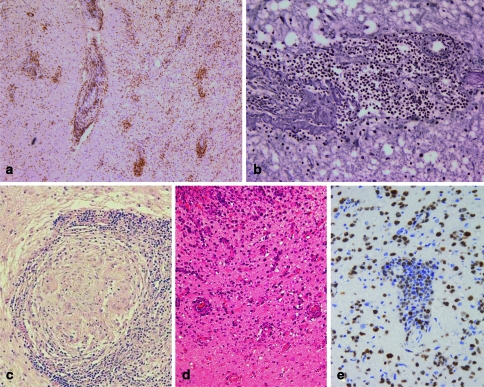
In vasculitis, the infiltrates are localized within the vessel wall and consist mostly of T cells [immunohistochemistry for the T cell marker CD3; (a)]. Frequently, the vessel wall is destroyed [reticulin staining; (b)]. Noncaseating granulomas consisting of multinucleated giant cells and epitheloid cells surrounded by a lymphocytic wall are the histological hallmarks of neurosarcoidosis (c). In CNS lymphomas, a perivascular accumulation of neoplastic B cells is characteristic [haematoxylin and eosin; (d)]. The high proliferation index in lymphomas may help to distinguish lymphomas from vasculitis or viral encephalitis. However, occasionally also cases of vasculitis and encephalitis show a marked proliferation. The detection of a monoclonal B cell population by PCR confirms the suspected diagnosis of a B cell lymphoma [immunohistochemistry for the proliferation marker Ki67; (e)]
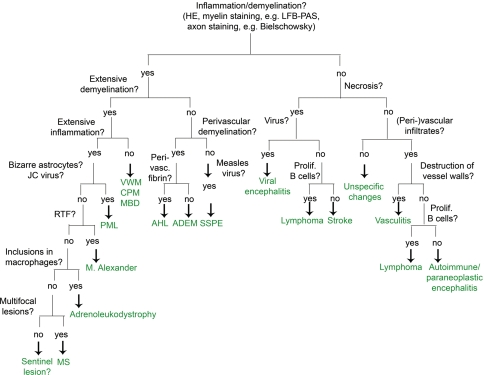
Flow chart for the diagnosis of MS and its most important differential diagnosis. ADEM acute disseminated encephalomyelitis, CPM central pontine myelinolysis, AHL acute haemorrhagic necrotizing leukoencephalitis; MBD Marchiafava-Bignami disease, MS multiple sclerosis, PML progressive multifocal leukoencephalopathy, RTF Rosenthal fibres, SSPE subacute sclerosing panencephalitis, VWM vanishing white matter disease
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/0002-9343(52)90234-9', 'is_inner': False, 'url': 'https://doi.org/10.1016/0002-9343(52)90234-9'}, {'type': 'PubMed', 'value': '14933429', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14933429/'}]}
- Adams RD, Kubik CS (1952) The morbid anatomy of demyelinative diseases. Am J Med 12:510–546 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '13616772', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/13616772/'}]}
- Adams RD, Victor M, Mancall EL (1959) Central pontine myelinolysis. A hitherto undescribed disease occurring in alcoholic and malnourished patients. Arch Neurol Psych 8138:154–172 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1002/1531-8249(200001)47:1<9::AID-ANA5>3.0.CO;2-I', 'is_inner': False, 'url': 'https://doi.org/10.1002/1531-8249(200001)47:1<9::aid-ana5>3.0.co;2-i'}, {'type': 'PubMed', 'value': '10632096', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10632096/'}]}
- Albert M, Austin L, Darnell R (2000) Detection and treatment of activated T cells in the cerebrospinal fluid of patients with paraneoplastic cerebellar degeneration. Ann Neurol 47:9–17 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1038/3315', 'is_inner': False, 'url': 'https://doi.org/10.1038/3315'}, {'type': 'PubMed', 'value': '9809559', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9809559/'}]}
- Albert M, Darnell J, Bender A, Francisco L, Bhardwaj N, Darnell R (1998) Tumor-specific killer cells in paraneoplastic cerebellar degeneration. Nat Med 4:1321–1324 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC486201', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC486201/'}, {'type': 'PubMed', 'value': '8558135', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8558135/'}]}
- Alderson L, Fetell MR, Sisti M, Hochberg F, Cohen M, Louis DN (1996) Sentinel lesions of primary CNS lymphoma. J Neurol Neurosurg Psychiatry 60:102–105 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
