

Estrogen receptor beta expression in nevi during pregnancy
- PMID: 18177352
- PMCID: PMC2766512
- DOI: 10.1111/j.1600-0625.2007.00667.x
Estrogen receptor beta expression in nevi during pregnancy
Abstract
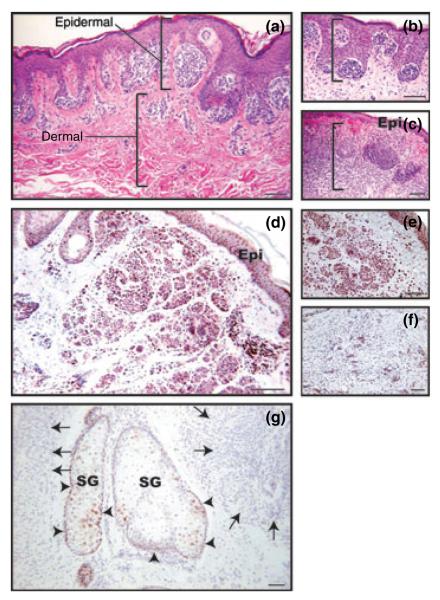
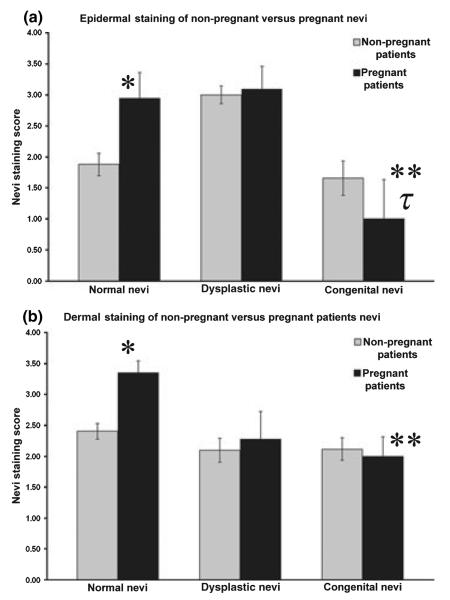
Estrogen levels increase during pregnancy and clinical evidence has long suggested that melanocytes are estrogen-responsive. We hypothesized that nevi from pregnant patients would exhibit increased expression of estrogen receptor beta (ERbeta) and thus enhanced potential to respond to altered estrogen levels. Normal, dysplastic and congenital nevi (n = 212) were collected from pregnant and non-pregnant women ranging from 18 to 45 years of age. Immunohistochemical staining was performed on these nevi using antibodies specifically directed against estrogen receptor alpha (ERalpha) and ERbeta. ERalpha was not observed in any lesions; thus, ERbeta was the predominant estrogen receptor in melanocytic cells from all types of nevi. Enhanced positivity for ERbeta in normal nevi during pregnancy was noted, compared with non-pregnant controls including nevocytes residing in both the epidermal and dermal micro-environments (P = 0.005 and P = 0.001 respectively). Nevi with increasingly melanocytic atypia showed increased ERbeta in nevocytes nested within the epidermis. No additional increase in ERbeta in atypical nevi was observed during pregnancy. For normal and congenital nevi, regardless of pregnancy status, dermally associated nevocytes tended to have greater ERbeta immunoreactivity. Significant decreases in ERbeta immunoreactivity were observed in congenital nevi from pregnant women compared with normal and dysplastic nevi from pregnant women. Our data suggest that nevi possess the capacity to be estrogen-responsive. Factors such as pregnancy and degree of atypia are associated with enhanced ERbeta with the exception of congenital nevi where the melanocytes were unique in their response to pregnancy.
Figures

References
-
- Elling SV, Powell FC. Physiological changes in the skin during pregnancy. Clin Dermatol. 1997;15:35–43. - PubMed
-
- Kroumpouzos G, Cohen LM. Dermatoses of pregnancy. J Am Acad Dermatol. 2001;45:1–19. quiz 19–22. - PubMed
-
- MacKelfresh J, Chen SC, Monthrope YM. Pregnancy and changes in melanocytic nevi. Obstet Gynecol. 2005;106:857–860. - PubMed
-
- Sanchez JL, Figueroa LD, Rodriguez E. Behavior of melanocytic nevi during pregnancy. Am J Dermatopathol. 1984;6(Suppl):89–91. - PubMed
-
- Zampino MR, Corazza M, Costantino D, Mollica G, Virgili A. Are melanocytic nevi influenced by pregnancy? A dermoscopic evaluation. Dermatol Surg. 2006;32:1497–1504. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
