

Review
doi: 10.1016/j.soc.2007.10.014.
Surgery for thyroid cancer
Affiliations
- PMID: 18177802
- PMCID: PMC4389794
- DOI: 10.1016/j.soc.2007.10.014
Item in Clipboard
Review
Surgery for thyroid cancer
Surg Oncol Clin N Am.
2008 Jan.
Abstract
A technique of thyroidectomy that facilitates resection of the thyroid, preserves the parathyroid glands with their blood supply, and preserves the recurrent and the superior laryngeal nerves is described. This technique provides a simple and versatile means of complete extracapsular thyroidectomy for lesions of the thyroid gland and minimizes postoperative complications.
Figures
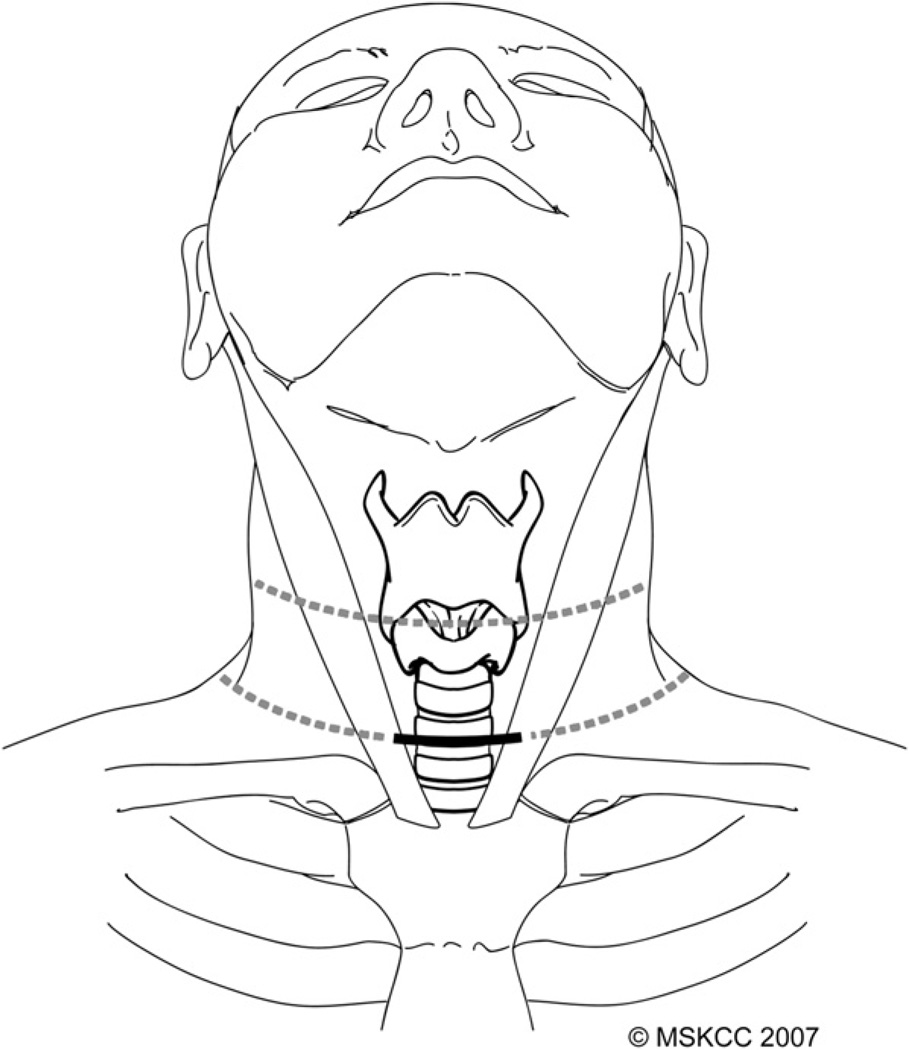
A transverse skin crease in the lower neck is chosen most commonly for the skin incision (bold line). This incision can be extended laterally if neck dissection is required or, alternatively, a higher skin crease can be selected (dotted lines). (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
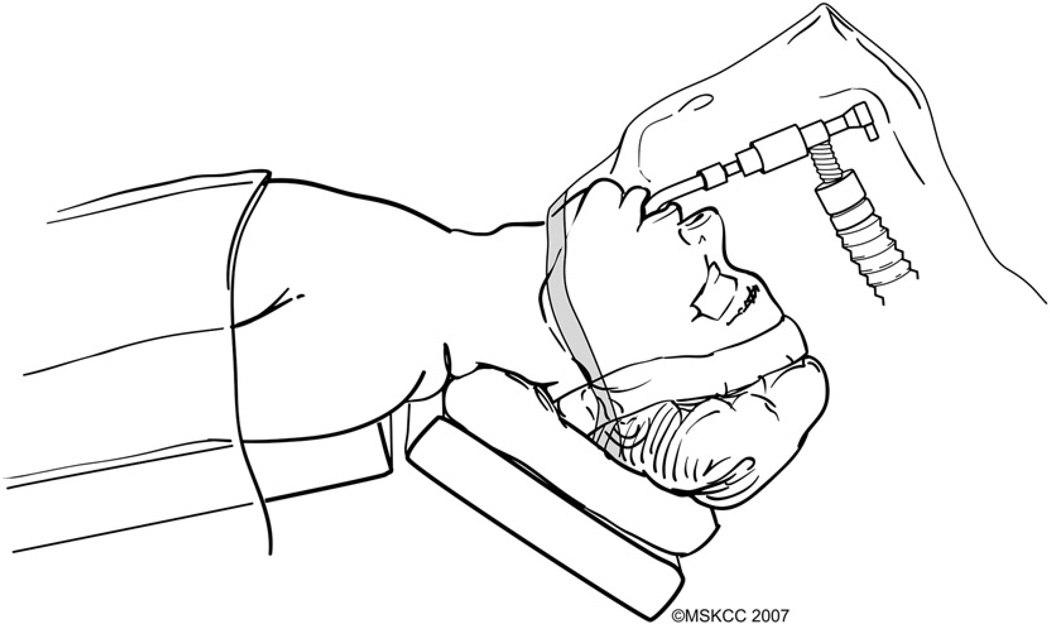
The patient is positioned supine on the operating table, which is maintained in a reverse Trendelenburg position with the neck extended. A transparent plastic drape allows continuous monitoring of the endotracheal tube and anesthesia circuit. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
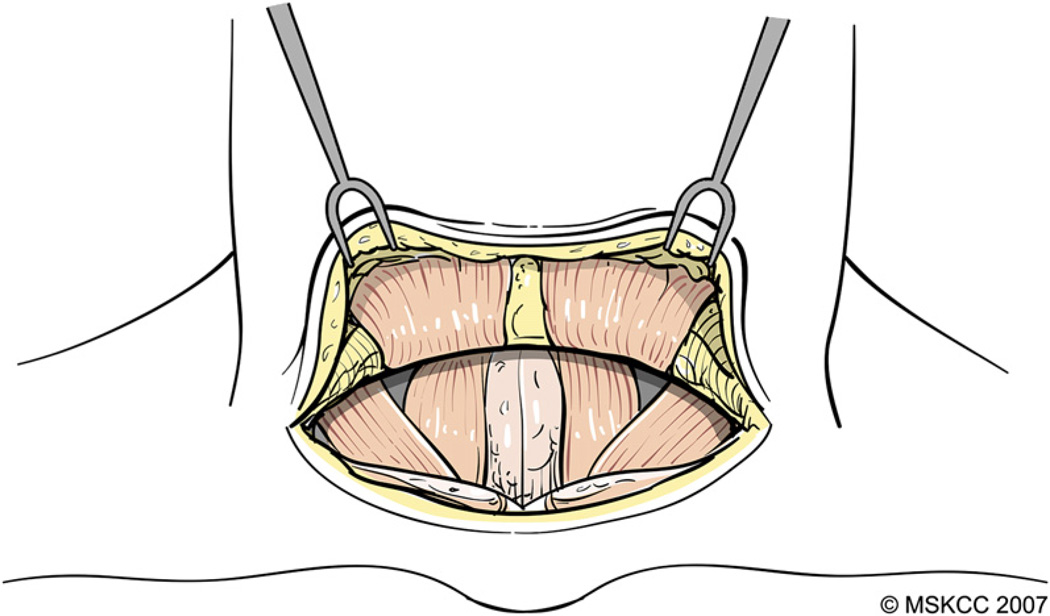
The platysma muscle is incised and cutaneous flaps are developed in the subplatysmal plane. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
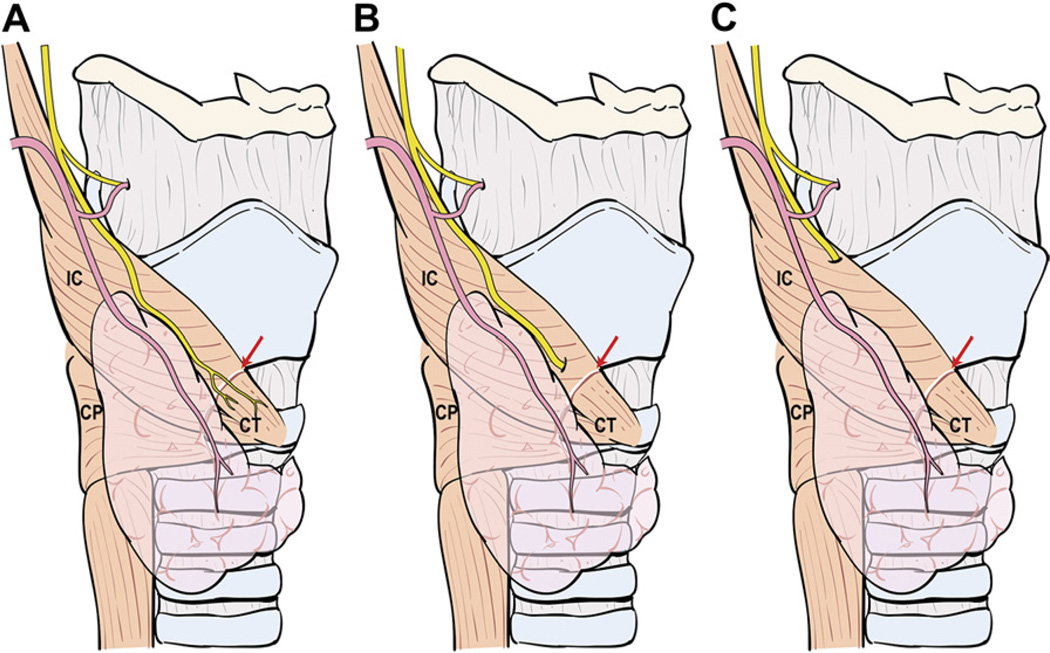
Variations in the anatomic relationship of the main trunk of the ESLN to the inferior constrictor (IC) muscle and superior thyroid pedicle. (A) The ESLN descends superficial to the IC muscle along the superior thyroid vessels so that it is visible in its entire course before innervating the cricothyroid (CT) muscle. (B) The ESLN pierces the IC muscle approximately 1 cm above the cricothyroid membrane (red arrow) so that only its upper portion is at risk for injury. (C) The ESLN runs deep to the IC muscle and, therefore, is protected from unintended injury during dissection in the vicinity of the superior thyroid pole. The cricopharyngeus muscle is marked CP.
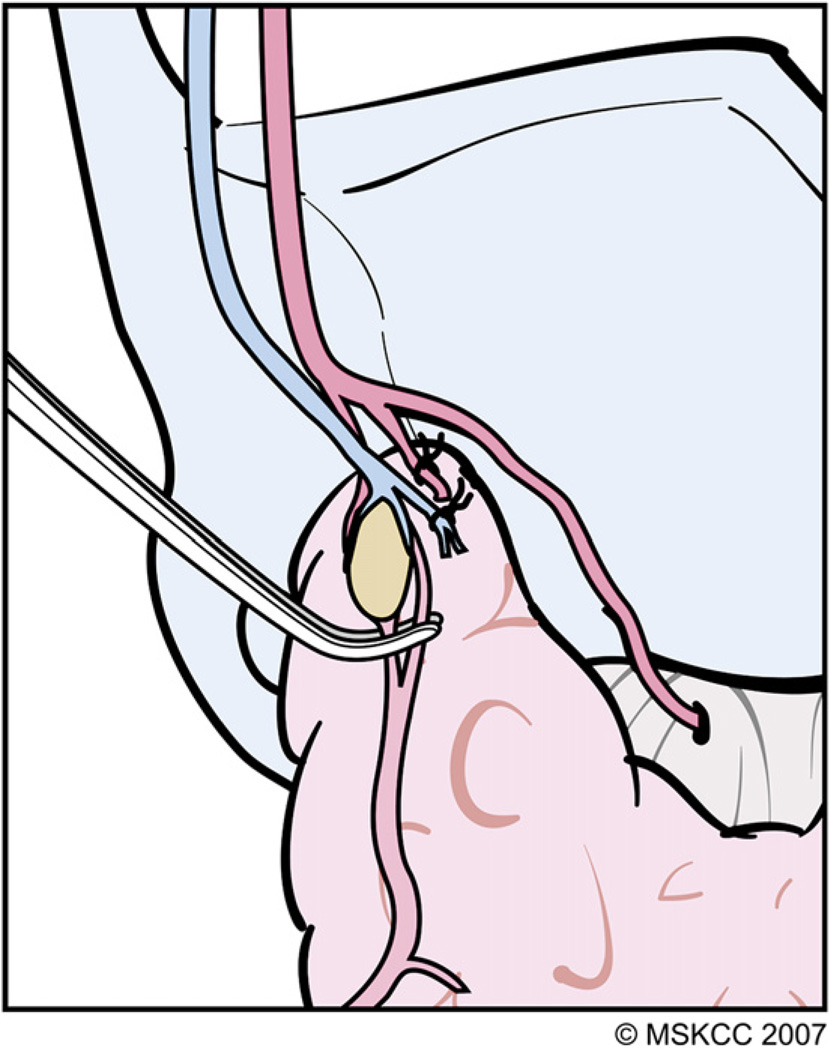
The technique of individual vessel ligation allows the surgeon to delineate the thyroid parenchymal tissue at the superior pole from its surrounding structures, minimizing risk for injury to the ESLN. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
As the superior pole tissue drops down away from the ESLN, the remaining small blood vessels, especially those in the vicinity of the superior PT gland, can be cauterized safely with fine-tipped bipolar electrocautery. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
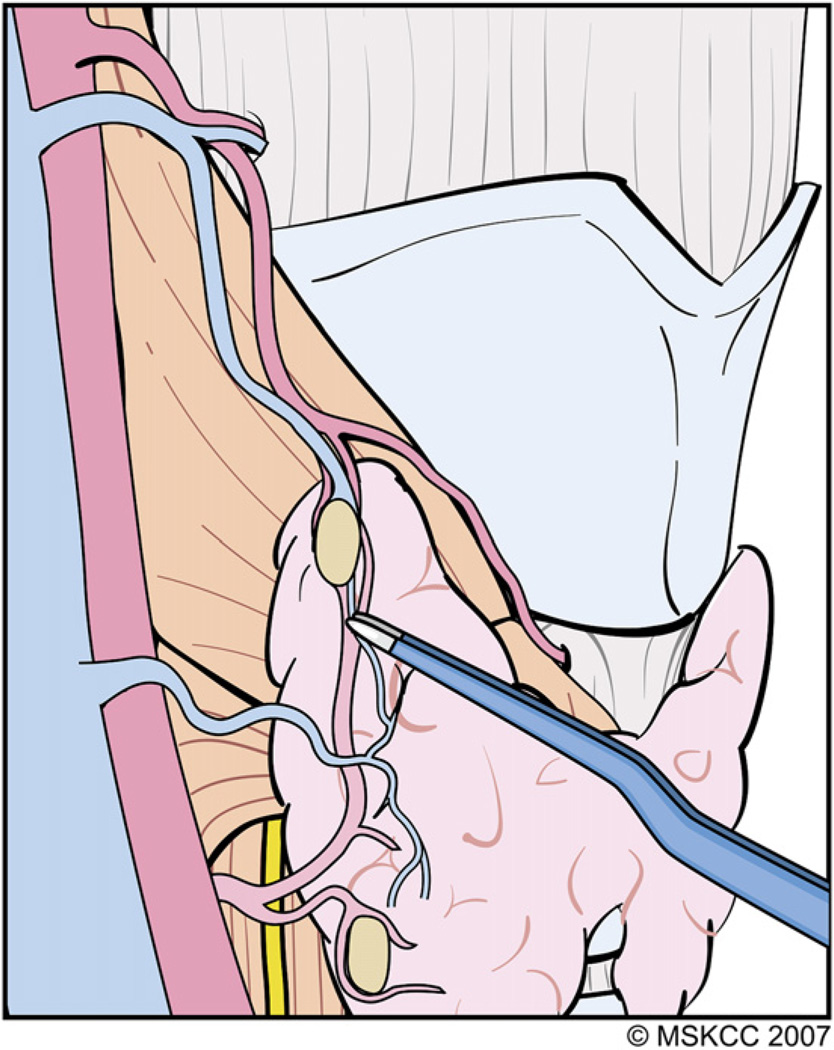
The PT glands receive their blood supply from branches of the ITA and, less frequently, from the superior thyroid artery. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
The terminal branches of the ITA that are encountered distal to the PT gland after they have supplied these glands are divided and ligated carefully. As the areolar tissue around the thyroid capsule is peeled away along with the PT gland, the RLN comes into view. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
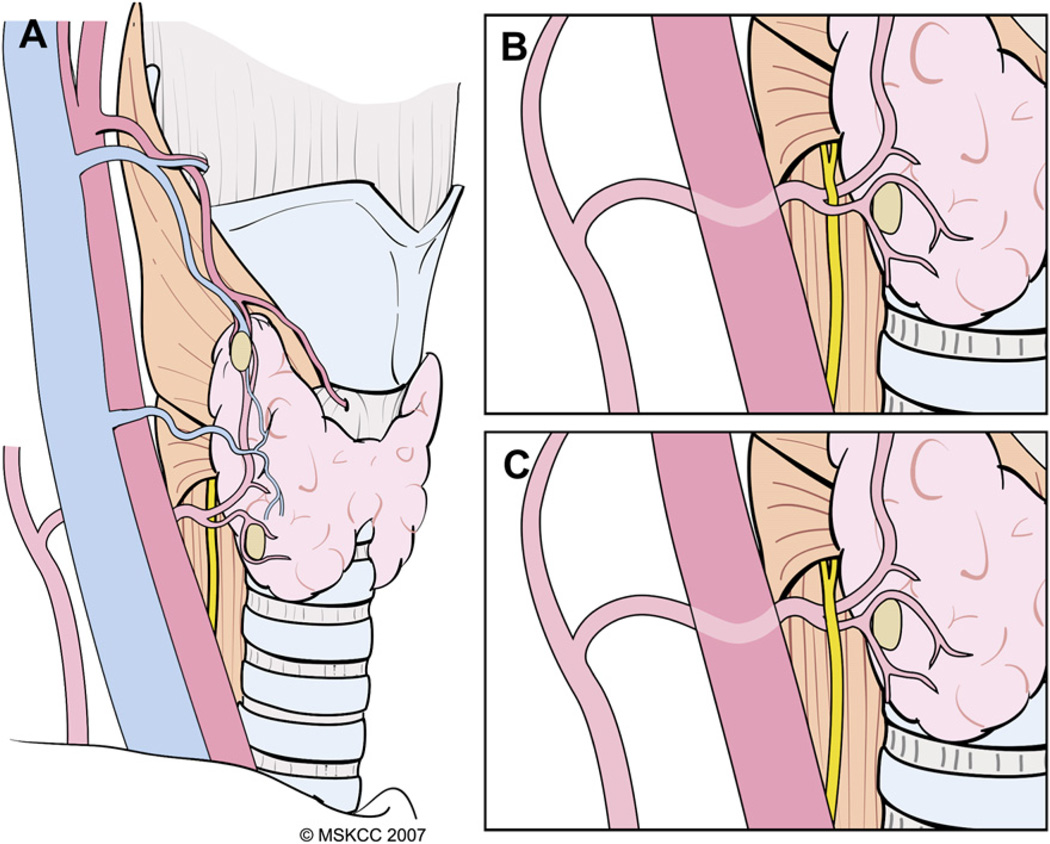
Variations in the relationship of the RLN to the ITA and its branches. Most commonly, the RLN courses deep to the inferior thyroid artery and its branches (A), but it may lie between the branches (B) or anterior (C) to the artery. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY.)
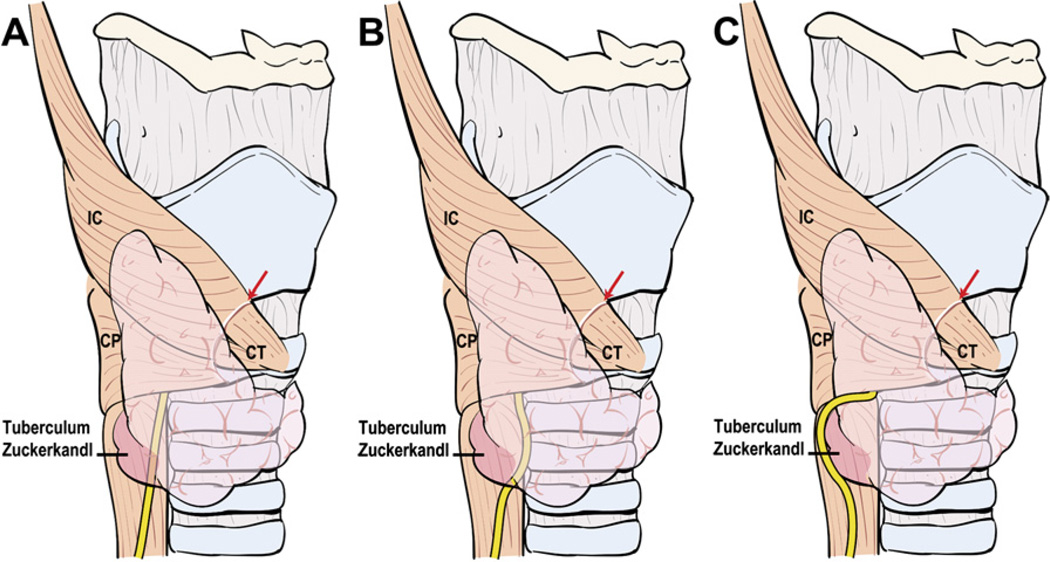
Variations in anatomic relationships of the RLN to the tuberculum Zuckerkandl. The RLN generally courses deep to the tuberculum Zuckerkandl and superficial to the lateral border of the trachea (A) but it may run medial to it (B). Nodular enlargement of thyroid tissue in the location of the tuberculum (C) may displace the RLN laterally around it, placing the nerve at risk for injury if this variation is not recognized. IC, inferior constrictor muscle; CP, cricopharyngeus muscle; CT, cricothyroid muscle.
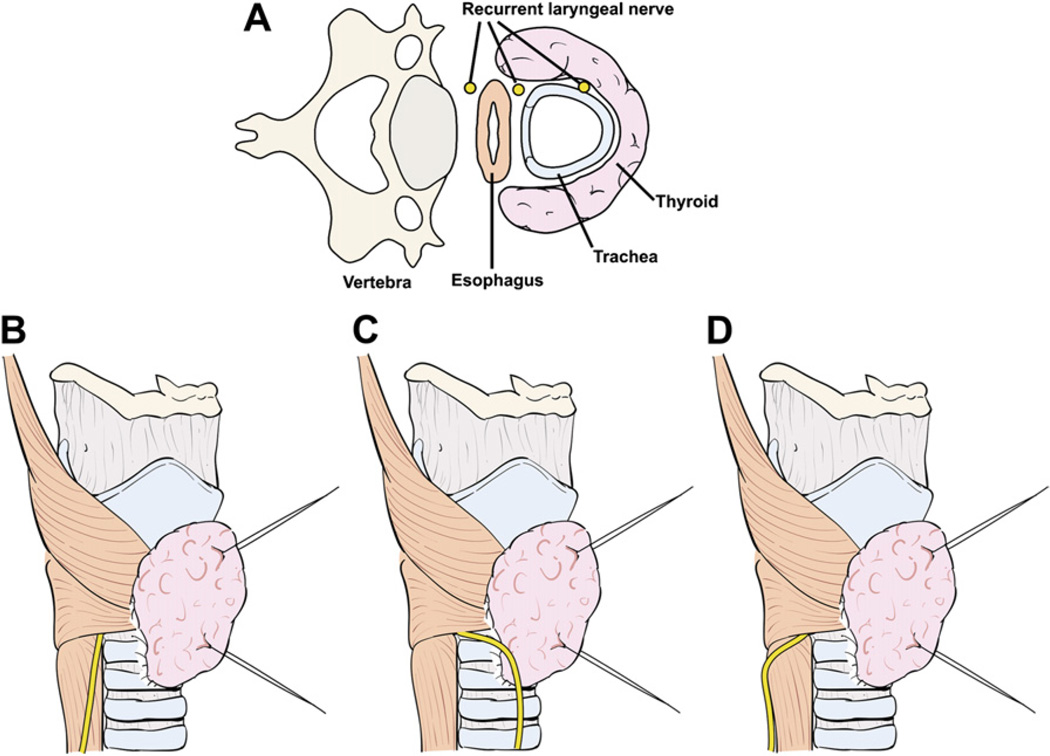
Anatomic relationship of the RLN to the tracheoesophageal groove (A). Most commonly, the RLN courses along the tracheoesophageal groove (B) and passes deep to Berry’s ligament. Variations include an RLN that ascends anterior to the tracheoesophageal groove (C) or along the paraesophageal line posterior to the tracheoesophageal groove (D).
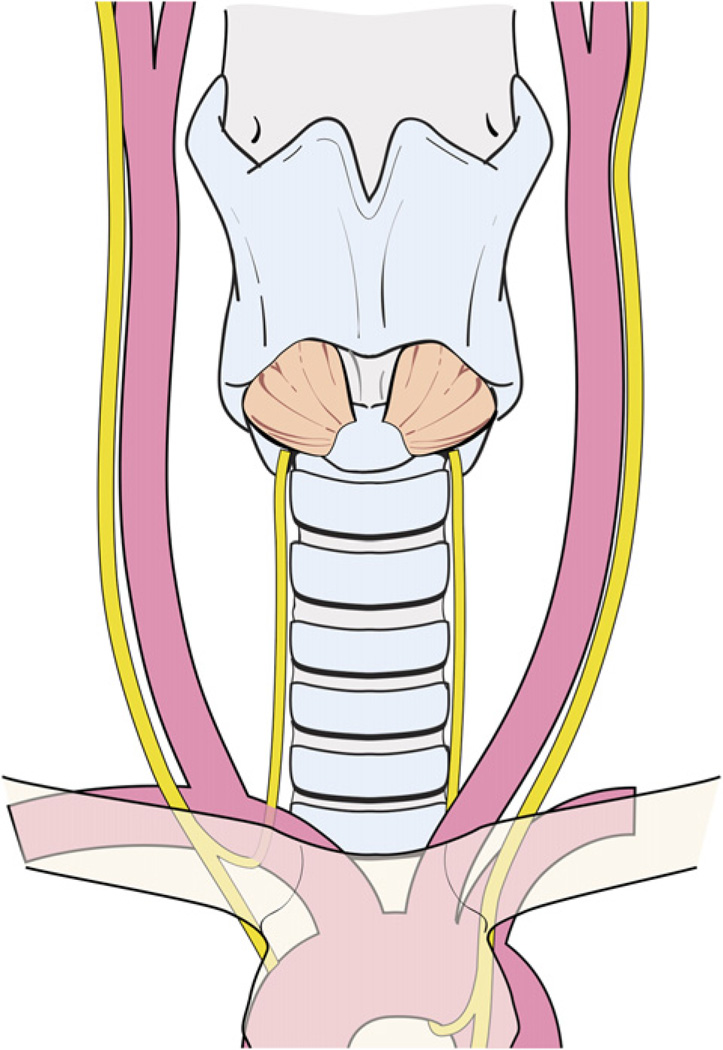
The left RLN crosses anterior to the aortic arch, loops under it, and ascends in a relatively constant position along the tracheoesophageal groove.
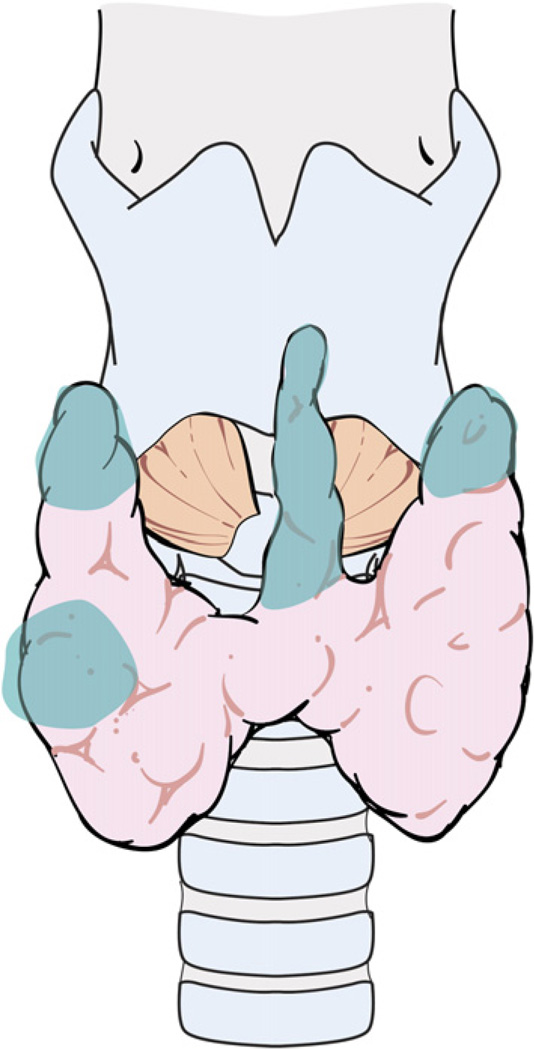
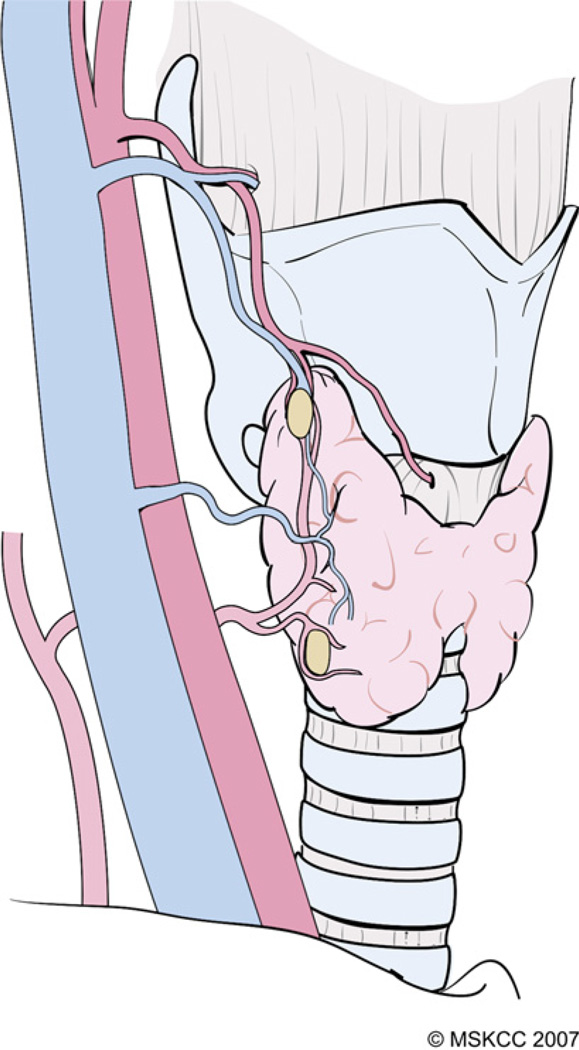
The common sites of residual thyroid tissue after total thyroidectomy are the superior poles, the thyroid tissue around Berry’s ligament, and the pyramidal lobe.
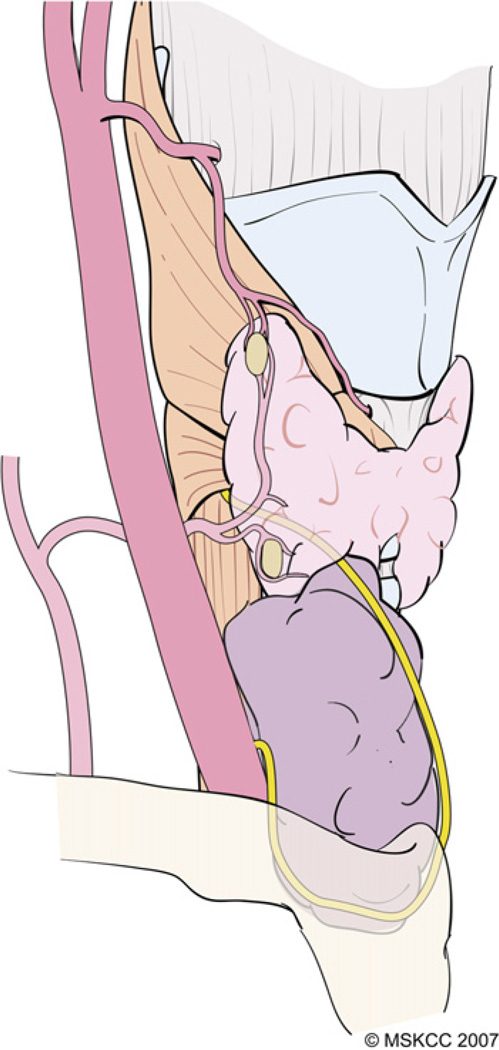
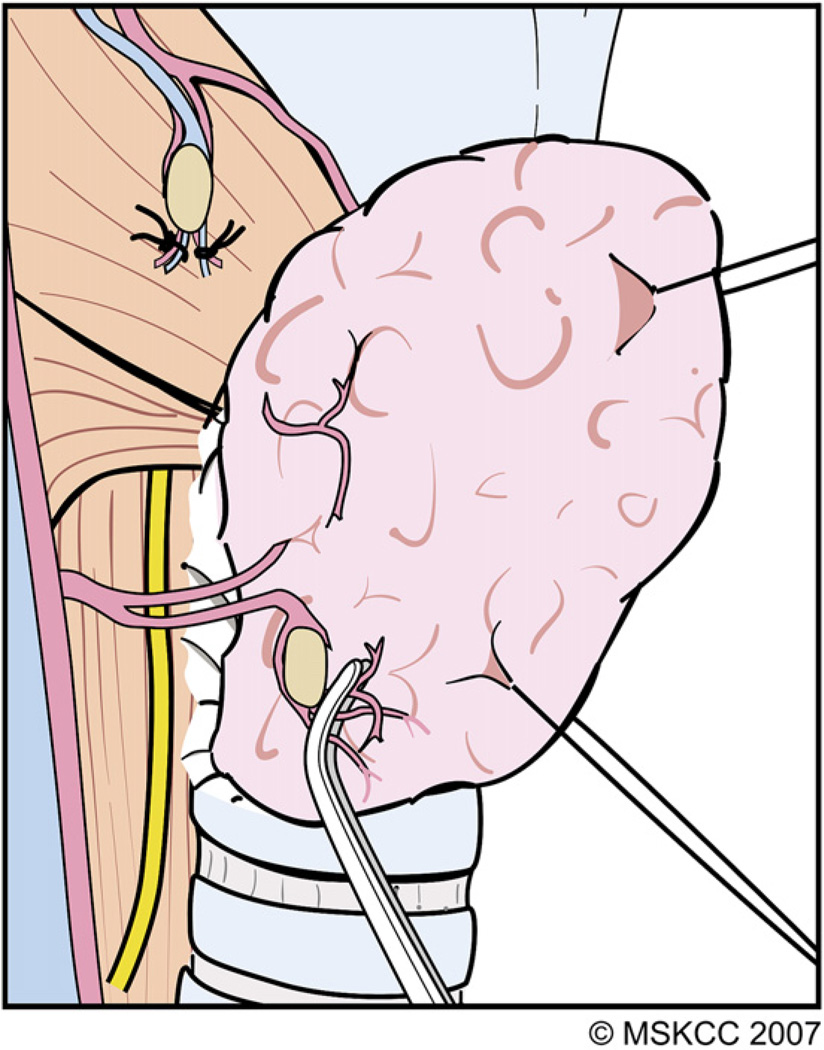
The RLN rarely may be displaced anteriorly if a nodule arises from a posterior location on the lower pole. If such a nodule extends retrosternally, attempts at delivery of the goiter outside of the wound before identifying the RLN places the nerve at significant risk, as it may be located more superficial than its usual location and is encountered early during the dissection. (Courtesy of the Memorial Sloan-Kettering Cancer Center, New York, NY; with permission.)
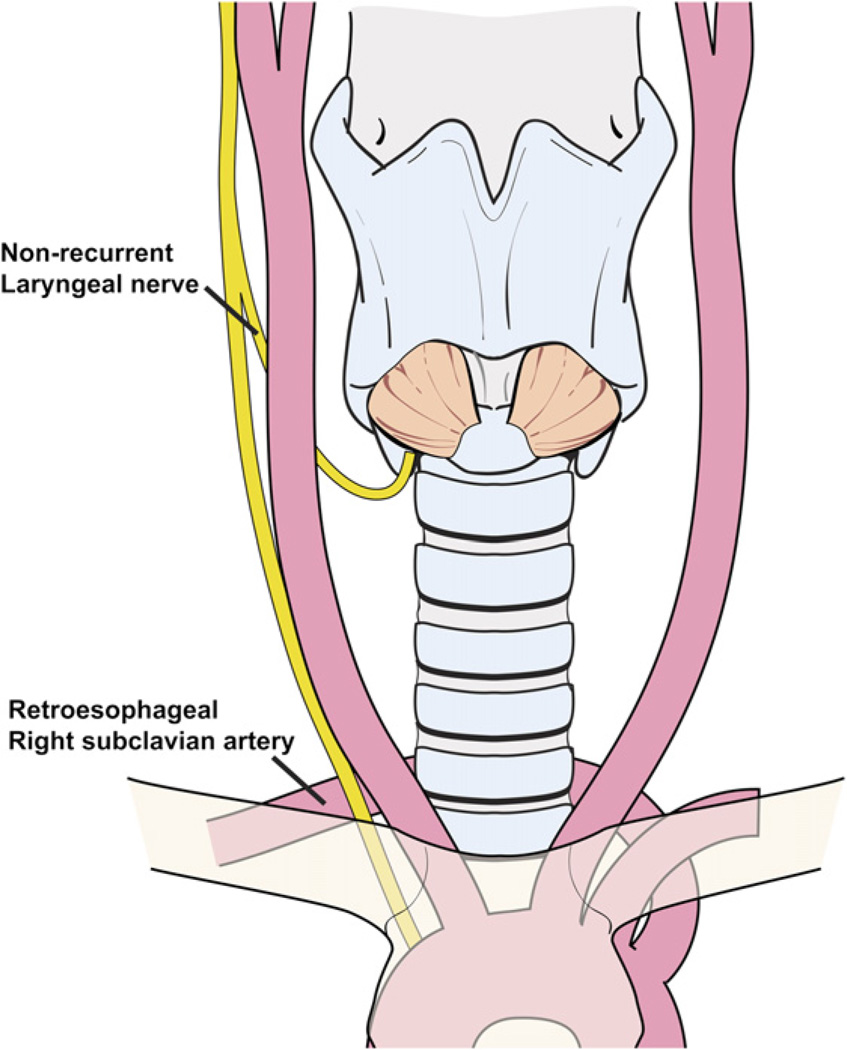
A nonrecurrent right laryngeal nerve occurs in patients who have a retroesophageal right subclavian artery.
References
-
- Newman E, Shaha AR. Substernal goiter. J Surg Oncol. 1995;60(3):207–212. - PubMed
-
- Johnson JT, Wagner RL. Infection following uncontaminated head and neck surgery. Arch Otolaryngol Head Neck Surg. 1987;113(4):368–369. - PubMed
-
- Friedman M, LoSavio P, Ibrahim H. Superior laryngeal nerve identification and preservation in thyroidectomy. Arch Otolaryngol Head Neck Surg. 2002;128(3):296–303. - PubMed
-
- Skandalakis JE, Droulias C, Harlaftis N, et al. The recurrent laryngeal nerve. AmSurg. 1976;42(9):629–634. - PubMed
-
- Blumberg NA. Observations on the pyramidal lobe of the thyroid gland. S Afr Med J. 1981;59(26):949–950. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
