

The OPTIMA study: assessing a new cinacalcet (Sensipar/Mimpara) treatment algorithm for secondary hyperparathyroidism
- PMID: 18178780
- PMCID: PMC2390975
- DOI: 10.2215/CJN.03591006
The OPTIMA study: assessing a new cinacalcet (Sensipar/Mimpara) treatment algorithm for secondary hyperparathyroidism
Abstract
Background and objectives: Cinacalcet, a novel calcimimetic, targets the calcium-sensing receptor to lower parathyroid hormone (PTH), calcium, and phosphorus levels in dialysis patients with secondary hyperparathyroidism (SHPT). This study compared the efficacy of a cinacalcet-based regimen with unrestricted conventional care (vitamin D and phosphate binders) for achieving the stringent National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) targets for dialysis patients.
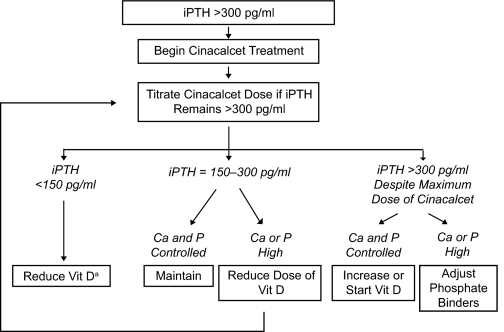
Study design: In this multicenter, open-label study, hemodialysis patients with poorly controlled SHPT were randomized to receive conventional care (n = 184) or a cinacalcet-based regimen (n = 368). Doses of cinacalcet, vitamin D sterols, and phosphate binders were adjusted during a 16-wk dose-optimization phase with the use of algorithms that allowed cinacalcet to be used with adjusted doses of vitamin D. The primary end point was the proportion of patients with mean intact PTH < or =300 pg/ml during a 7-wk efficacy assessment phase.
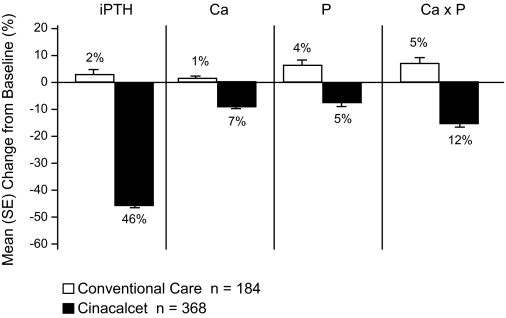
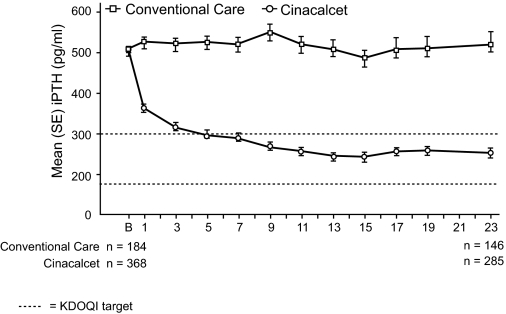
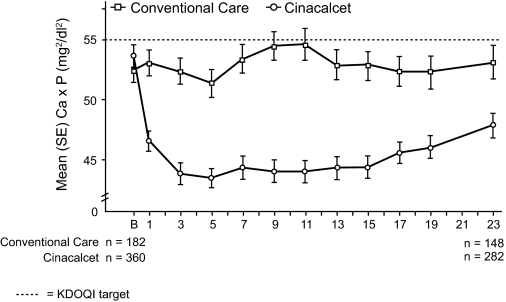
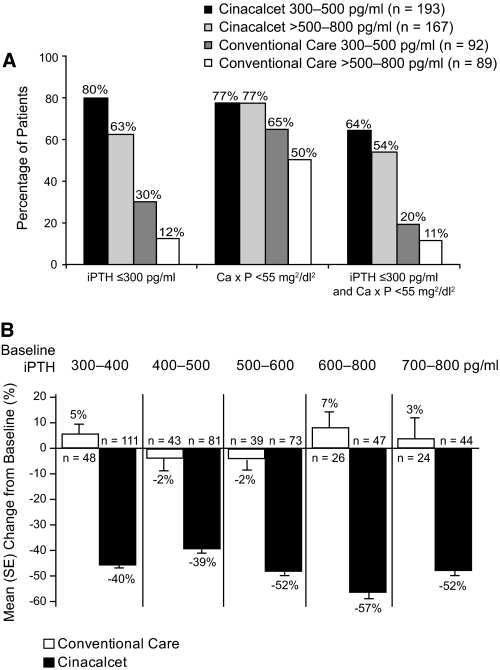
Results: A higher proportion of patients receiving the cinacalcet-based regimen versus conventional care achieved the targets for PTH (71% versus 22%, respectively; P < 0.001), Ca x P (77% versus 58%, respectively; P < 0.001), calcium (76% versus 33%, respectively; P < 0.001), phosphorus (63% versus 50%, respectively; P = 0.002), and PTH and Ca x P (59% versus 16%, respectively, P < 0.001), and allowed a 22% reduction in vitamin D dosage in patients receiving vitamin D at baseline. Achievement of targets was greatest in patients with less severe disease (intact PTH range, 300 to 500 pg/ml) and the cinacalcet dose required was lower in these patients (median = 30 mg/d).
Conclusions: Compared with conventional therapy, a cinacalcet-based treatment algorithm increased achievement of KDOQI treatment targets in dialysis patients in whom conventional therapy was no longer effective in controlling this disease.
Figures
References
-
- Martinez I, Saracho R, Montenegro J, Liach F: The importance of dietary calcium and phosphorus in the secondary hyperparathyroidism of patients with early renal failure. Am J Kidney Dis 29: 496–502, 1997 - PubMed
-
- Slatopolsky E, Brown A, Dusso A: Pathogenesis of secondary hyperparathyroidism. Kidney Int 56[Suppl 73]: S14–S19, 1999 - PubMed
-
- Salem MM: Hyperparathyroidism in the dialysis population: a survey of 612 patients. Am J Kidney Dis 29: 862–865, 1997 - PubMed
-
- Billa V, Zhong A, Bargman J, Vas S, Wong PY, Oreopoulos DG: High prevalence of hyperparathyroidism among peritoneal dialysis patients: A review of 176 patients. Perit Dial Int 20: 315–321, 2000 - PubMed
-
- Hruska KA, Teitelbaum SL: Renal osteodystrophy. N Engl J Med 333: 166–174, 1995 - PubMed
