

22q11.2 distal deletion: a recurrent genomic disorder distinct from DiGeorge syndrome and velocardiofacial syndrome
- PMID: 18179902
- PMCID: PMC2253964
- DOI: 10.1016/j.ajhg.2007.09.014
22q11.2 distal deletion: a recurrent genomic disorder distinct from DiGeorge syndrome and velocardiofacial syndrome
Abstract
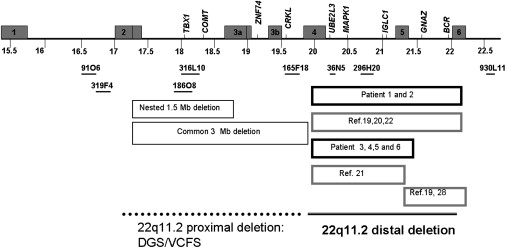
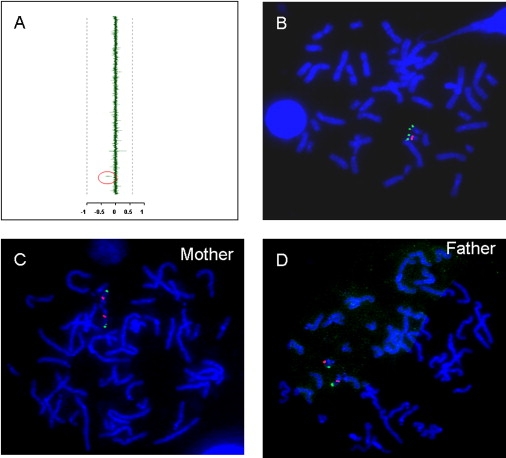
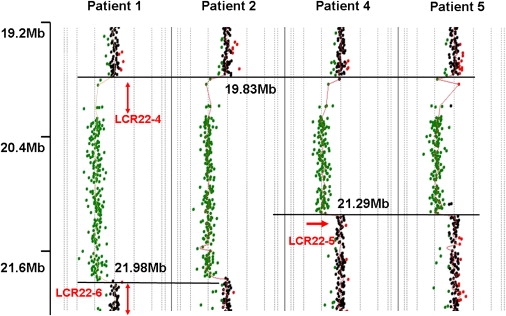
Microdeletions within chromosome 22q11.2 cause a variable phenotype, including DiGeorge syndrome (DGS) and velocardiofacial syndrome (VCFS). About 97% of patients with DGS/VCFS have either a common recurrent approximately 3 Mb deletion or a smaller, less common, approximately 1.5 Mb nested deletion. Both deletions apparently occur as a result of homologous recombination between nonallelic flanking low-copy repeat (LCR) sequences located in 22q11.2. Interestingly, although eight different LCRs are located in proximal 22q, only a few cases of atypical deletions utilizing alternative LCRs have been described. Using array-based comparative genomic hybridization (CGH) analysis, we have detected six unrelated cases of deletions that are within 22q11.2 and are located distal to the approximately 3 Mb common deletion region. Further analyses revealed that the rearrangements had clustered breakpoints and either a approximately 1.4 Mb or approximately 2.1 Mb recurrent deletion flanked proximally by LCR22-4 and distally by either LCR22-5 or LCR22-6, respectively. Parental fluorescence in situ hybridization (FISH) analyses revealed that none of the available parents (11 out of 12 were available) had the deletion, indicating de novo events. All patients presented with characteristic facial dysmorphic features. A history of prematurity, prenatal and postnatal growth delay, developmental delay, and mild skeletal abnormalities was prevalent among the patients. Two patients were found to have a cardiovascular malformation, one had truncus arteriosus, and another had a bicuspid aortic valve. A single patient had a cleft palate. We conclude that distal deletions of chromosome 22q11.2 between LCR22-4 and LCR22-6, although they share some characteristic features with DGS/VCFS, represent a novel genomic disorder distinct genomically and clinically from the well-known DGS/VCF deletion syndromes.
Figures

References
-
- Scambler P.J. The 22q11 deletion syndromes. Hum. Mol. Genet. 2000;9:2421–2426. - PubMed
-
- Shprintzen R.J., Goldberg R.B., Lewin M.L., Sidoti E.J., Berkman M.D., Argamaso R.V., Young D. A new syndrome involving cleft palate, cardiac anomalies, typical facies, and learning disabilities: velo-cardio-facial syndrome. Cleft Palate J. 1978;15:56–62. - PubMed
-
- Emanuel B.S., McDonald-McGinn D., Saitta S.C., Zackai E.H. The 22q11.2 deletion syndrome. Adv. Pediatr. 2001;48:39–73. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
