

Early versus late intravenous insulin administration in critically ill patients
- PMID: 18180902
- PMCID: PMC2486366
- DOI: 10.1007/s00134-007-0978-3
Early versus late intravenous insulin administration in critically ill patients
Abstract
Objective: To investigate whether timing of intensive insulin therapy (IIT) after intensive care unit (ICU) admission influences outcome.
Design and setting: Single-center prospective cohort study in the 14-bed medical ICU of a 1,171-bed tertiary teaching hospital.
Patients: The study included 127 patients started on ITT within 48 h of ICU admission (early group) and 51 started on ITT thereafter (late group); the groups did not differ in age, gender, race, BMI, APACHE III, ICU steroid use, admission diagnosis, or underlying comorbidities.
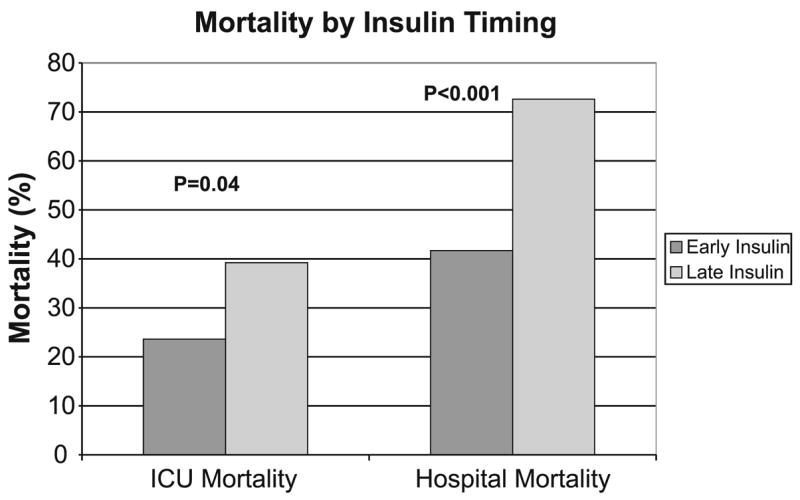
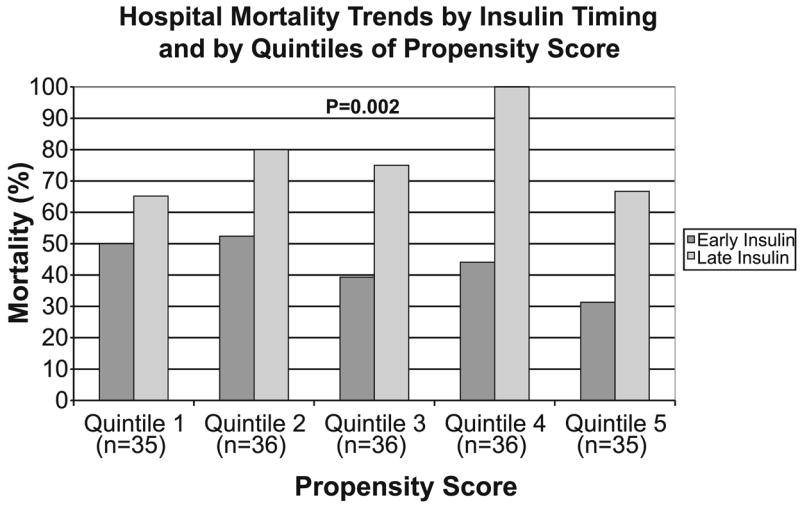
Measurements and results: The early group had more ventilator-free days in the first 28 days after ICU admission (median 12 days, IQR 0-24, vs. 1 day, 0-11), shorter ICU stay (6 days, IQR 3-11, vs. 11 days, vs. 7-17), shorter hospital stay (15 days, IQR 9-30, vs. 25 days, 13-43), lower ICU mortality (OR 0.48), and lower hospital mortality (OR 0.27). On multivariate analysis, early therapy was still associated with decreased hospital mortality (ORadj 0.29). The strength and direction of association favoring early IIT was consistent after propensity score modeling regardless of method used for analysis.
Conclusions: Early IIT was associated with better outcomes. Our results raise questions about the assumption that delayed administration of IIT has the same benefit as early therapy. A randomized study is needed to determine the optimal timing of therapy.
Figures
References
-
- Bernard C. Leçons sur le Diabète. Paris: 1877.
-
- Cely CM, Arora P, Quartin AA, Kett DH, Schein RM. Relationship of baseline glucose homeostasis to hyperglycemia during medical critical illness. Chest. 2004;126:879–887. - PubMed
-
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78:1471–1478. - PubMed
-
- Laird AM, Miller PR, Kilgo PD, Meredith JW, Chang MC. Relationship of early hyperglycemia to mortality in trauma patients. J Trauma. 2004;56:1058–1062. - PubMed
-
- Bjerke HS, Shabot MM. Glucose intolerance in critically ill surgical patients: relationship to total parenteral nutrition and severity of illness. Am Surg. 1992;58:728–731. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
