

Population pharmacokinetic model for docetaxel in patients with varying degrees of liver function: incorporating cytochrome P4503A activity measurements
- PMID: 18183036
- PMCID: PMC3092481
- DOI: 10.1038/sj.clpt.6100476
Population pharmacokinetic model for docetaxel in patients with varying degrees of liver function: incorporating cytochrome P4503A activity measurements
Abstract
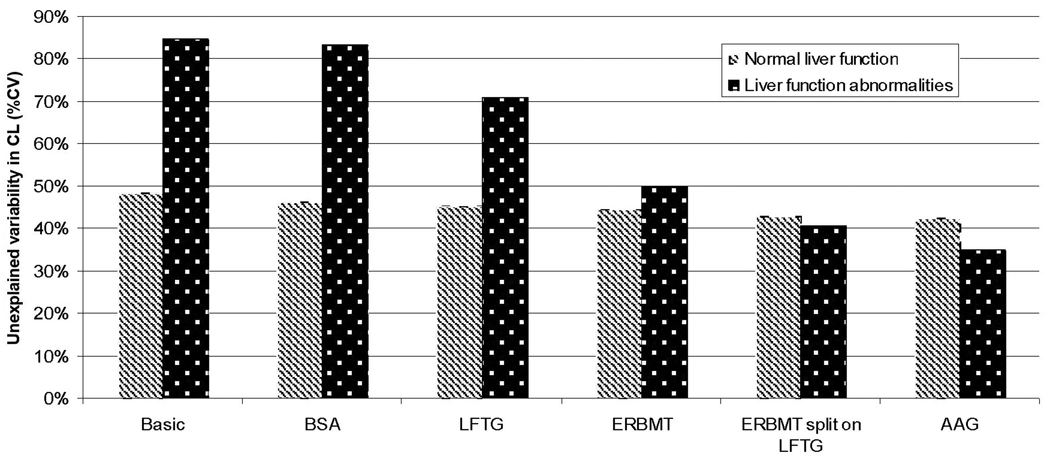
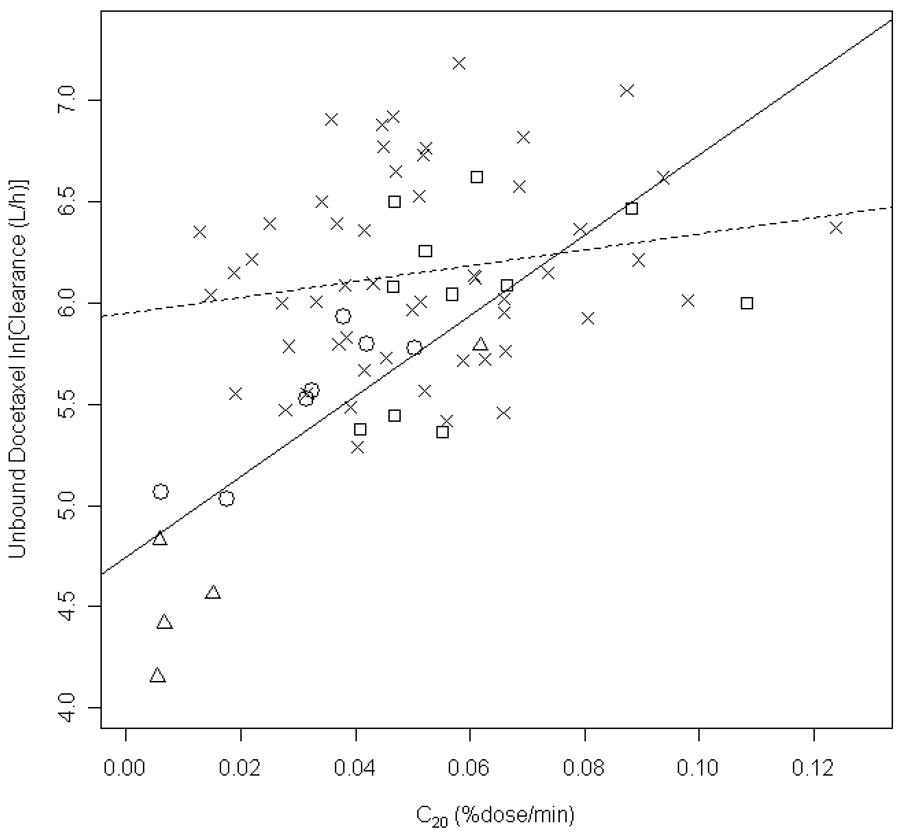
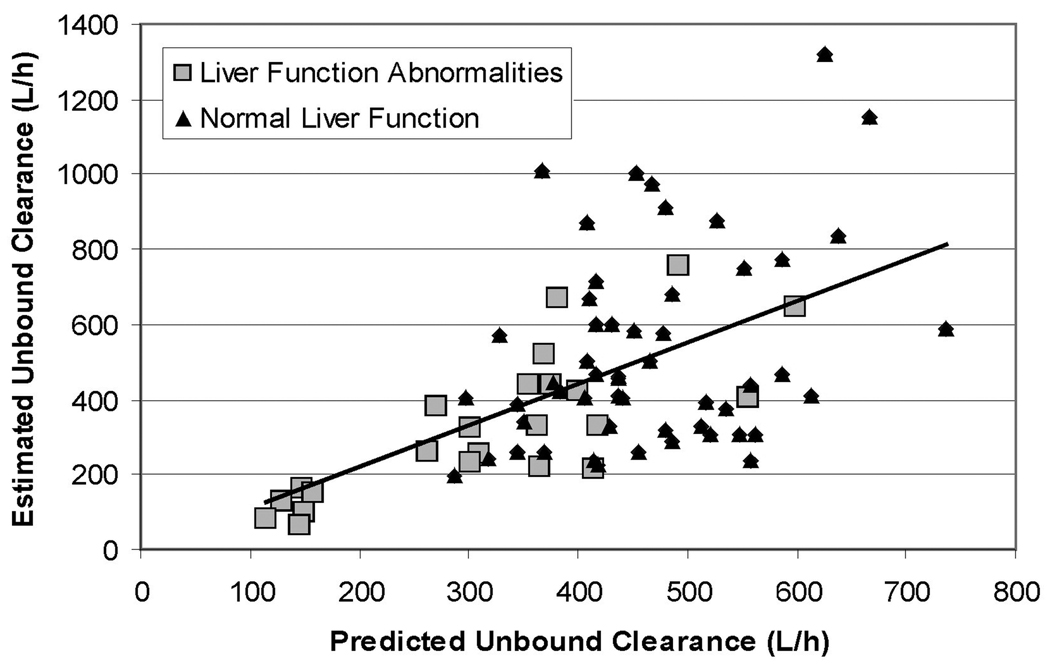
The relationship between cytochrome P4503A4 (CYP3A4) activity and docetaxel clearance in patients with varying degrees of liver function (LF) was evaluated. Docetaxel 40, 50, or 75 mg/m(2) was administered to 85 patients with advanced cancer; 23 of 77 evaluable patients had abnormalities in LF tests. Baseline CYP3A activity was assessed using the erythromycin breath test (ERMBT). Pharmacokinetic studies and toxicity assessments were performed during cycle 1 of therapy and population modeling was performed using NONMEM. Docetaxel unbound clearance was lower (317 vs. 470 l/h) and more variable in patients with LF abnormalities compared to patients with normal LF. Covariates evaluated accounted for 83% of variability on clearance in patients with liver dysfunction, with CYP3A4 activity accounting for 47% of variation; covariates accounted for only 23% of variability in patients with normal LF. The clinical utility of the ERMBT may lie in identifying safe docetaxel doses for patients with LF abnormalities.
Conflict of interest statement
Dr. Carducci is a consultant to and on the speaker’s bureau for Sanofi-Aventis.
Figures

References
-
- Bruno R, Hille D, Riva A, Vivier N, ten Bokkel Huinnink WW, van Oosterom AT, et al. Population pharmacokinetics/pharmacodynamics of docetaxel in phase II studies in patients with cancer. Journal of Clinical Oncology. 1998;16:187–196. - PubMed
-
- Bruno R, Vivier N, Veyrat-Follet C, Montay G, Rhodes GR. Population pharmacokinetics and pharmacokinetic-pharmacodynamic relationships for docetaxel. Invest New Drugs. 2001;19:163–169. - PubMed
-
- Bruno R, Olivares R, Berille J, Chaikin P, Vivier N, Hammershaimb L, et al. Alpha-1-acid glycoprotein as an independent predictor for treatment effects and a prognostic factor of survival in patients with non-small cell lung cancer treated with docetaxel. Clin Cancer Res. 2003;9:1077–1082. - PubMed
-
- Shou M, Martinet M, Korzekwa KR, Krausz KW, Gonzalez FJ, Gelboin HV. Role of human cytochrome P450 3A4 and 3A5 in the metabolism of taxotere and its derivatives: enzyme specificity, interindividual distribution and metabolic contribution in human liver. Pharmacogenetics. 1998;8:391–401. - PubMed
-
- Baker SD, Sparreboom A, Verweij J. Clinical pharmacokinetics of docetaxel : recent developments. Clin Pharmacokinet. 2006;45:235–252. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
