

Feasibility of reducing the duration of placebo-controlled trials in schizophrenia research
- PMID: 18184634
- PMCID: PMC2632413
- DOI: 10.1093/schbul/sbm152
Feasibility of reducing the duration of placebo-controlled trials in schizophrenia research
Abstract
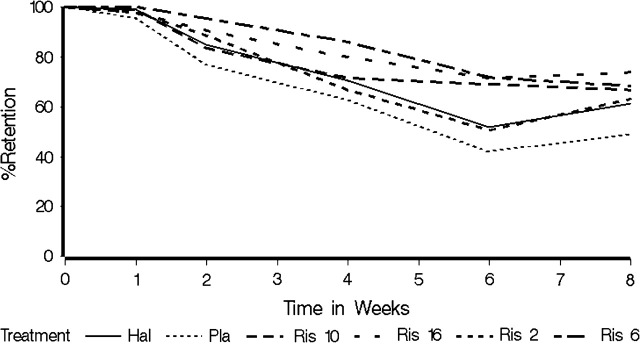
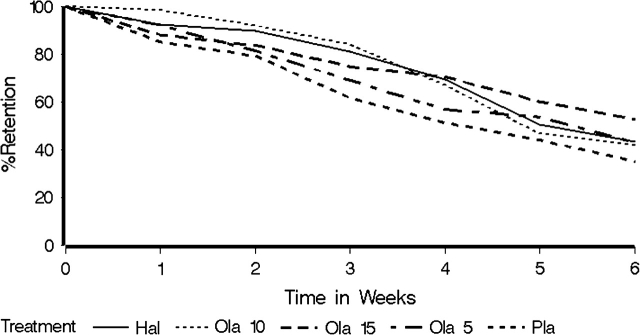
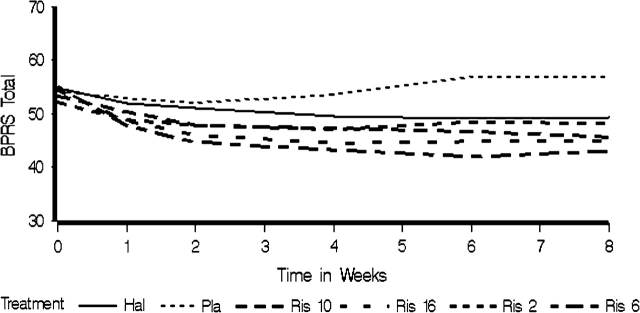
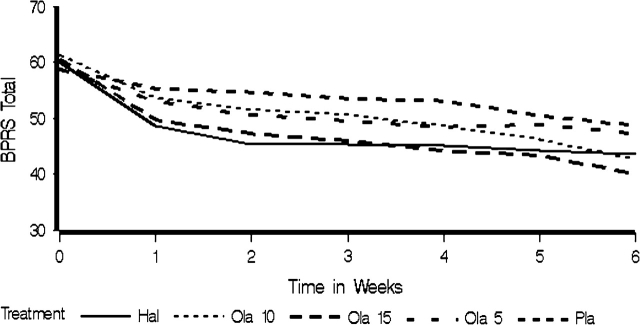
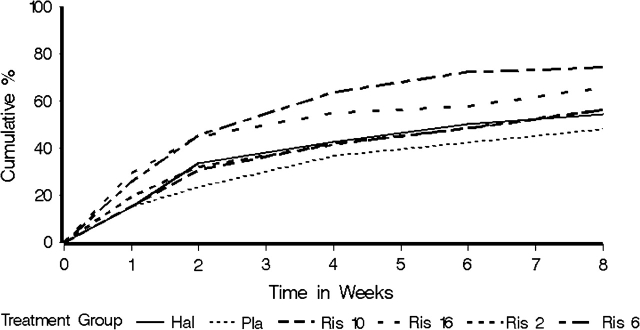
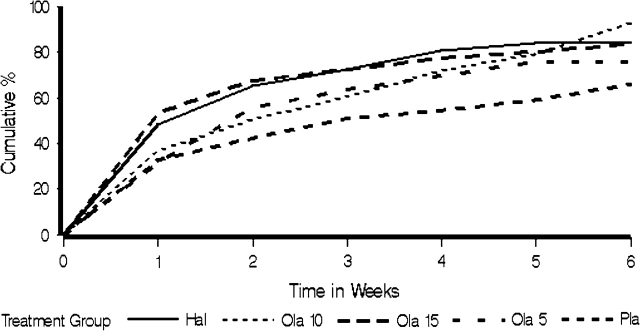
Use of placebo-controlled trials in medical and psychiatric research has been controversial, although a consensus is emerging about conditions under which placebo-controlled trials are ethical. In schizophrenia research, the paradigm of slow onset of antipsychotic effects has led to a model in which placebo-controlled trials of 6-8 weeks duration have been used to demonstrate efficacy. Recent evidence that the largest symptom reductions are typically seen in the first weeks of treatment suggests that shorter placebo-controlled studies to demonstrate antipsychotic efficacy are possible. In a pilot study of the feasibility of shortening placebo-controlled studies, we reanalyzed data from placebo-controlled registry trials of olanzapine and risperidone and found that trials as short as 4 weeks could have similar power to longer term 6-8 week studies, given the estimated time course of treatment effects. Although fuller evaluation is required, the results suggest future antipsychotic trials could be shortened from 6-8 weeks to 3-4 weeks with a relatively low increase in sample size requirements. Shortening placebo-controlled trials would reduce patient burden and ethical objections to prolonged administration of placebo and reduce potential bias due to high dropout rates in longer clinical trials.
Figures
Similar articles
-
Joint modeling of dropout and outcome in three pivotal clinical trials of schizophrenia.Schizophr Res. 2015 May;164(1-3):122-6. doi: 10.1016/j.schres.2015.02.021. Epub 2015 Mar 16. Schizophr Res. 2015. PMID: 25790904
-
Dropout rates in placebo-controlled and active-control clinical trials of antipsychotic drugs: a meta-analysis.Arch Gen Psychiatry. 2005 Dec;62(12):1305-12. doi: 10.1001/archpsyc.62.12.1305. Arch Gen Psychiatry. 2005. PMID: 16330718
-
Predictors of antipsychotic-induced weight gain in first-episode psychosis: conclusions from a randomized, double-blind, controlled prospective study of olanzapine, risperidone, and haloperidol.J Clin Psychopharmacol. 2008 Feb;28(1):27-31. doi: 10.1097/jcp.0b013e3181602fe6. J Clin Psychopharmacol. 2008. PMID: 18204337 Clinical Trial.
-
Control group bias in randomized atypical antipsychotic medication trials for schizophrenia.Arch Gen Psychiatry. 2005 Sep;62(9):961-70. doi: 10.1001/archpsyc.62.9.961. Arch Gen Psychiatry. 2005. PMID: 16143728 Review.
-
Atypical antipsychotics in elderly patients with dementia or schizophrenia: review of recent literature.Harv Rev Psychiatry. 2005 Nov-Dec;13(6):340-51. doi: 10.1080/10673220500433247. Harv Rev Psychiatry. 2005. PMID: 16373328 Review.
Cited by
-
Are Randomized Controlled Trials on Pharmacotherapy and Psychotherapy for Positive Symptoms of Schizophrenia Comparable? A Systematic Review of Patient and Study Characteristics.Schizophr Bull. 2020 Apr 10;46(3):496-504. doi: 10.1093/schbul/sbz090. Schizophr Bull. 2020. PMID: 32275756 Free PMC article.
-
Predictors of Placebo Response in Pharmacological Clinical Trials of Negative Symptoms in Schizophrenia: A Meta-regression Analysis.Schizophr Bull. 2019 Jan 1;45(1):57-68. doi: 10.1093/schbul/sbx192. Schizophr Bull. 2019. PMID: 29370436 Free PMC article.
-
Trace amine-associated receptor 1 (TAAR1) agonists for psychosis: protocol for a living systematic review and meta-analysis of human and non-human studies.Wellcome Open Res. 2023 Aug 25;8:365. doi: 10.12688/wellcomeopenres.19866.1. eCollection 2023. Wellcome Open Res. 2023. PMID: 38634067 Free PMC article.
-
Comparative efficacy and tolerability of 32 oral antipsychotics for the acute treatment of adults with multi-episode schizophrenia: a systematic review and network meta-analysis.Lancet. 2019 Sep 14;394(10202):939-951. doi: 10.1016/S0140-6736(19)31135-3. Epub 2019 Jul 11. Lancet. 2019. PMID: 31303314 Free PMC article.
-
Structural models describing placebo treatment effects in schizophrenia and other neuropsychiatric disorders.Clin Pharmacokinet. 2011 Jul;50(7):429-50. doi: 10.2165/11590590-000000000-00000. Clin Pharmacokinet. 2011. PMID: 21651312
References
-
- Kemmler G, Hummer M, Widschwendter C, Fleischhacker WW. Dropout rates in placebo-controlled and active-control clinical trials of antipsychotic drugs: a meta-analysis. Arch Gen Psychiatry. 2005;62:1305–1312. - PubMed
-
- Leber P. The use of placebo control groups in the assessment of psychiatric drugs: an historical context. Biol Psychiatry. 2000;47:699–706. - PubMed
-
- Aras G. Superiority, noninferiority, equivalence and bioequivalence-revisitied. Drug Inf J. 2001;35:1157–1164.
-
- Streiner DL. Alternatives to placebo-controlled trials. Can J Neurol Sci. 2007;34(suppl 1):S37–S41. - PubMed
-
- Weijer C. Placebo-controlled trials in schizophrenia: are they ethical? Are they necessary? Schizophr Res. 1999;35:211–218. discussion 227–236. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
