

Selective single blastocyst transfer reduces the multiple pregnancy rate and increases pregnancy rates: a pre- and postintervention study
- PMID: 18190376
- PMCID: PMC2253713
- DOI: 10.1111/j.1471-0528.2007.01584.x
Selective single blastocyst transfer reduces the multiple pregnancy rate and increases pregnancy rates: a pre- and postintervention study
Abstract
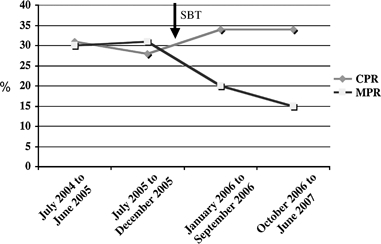
Objective: To examine the clinical pregnancy rate (CPR) and multiple pregnancy rate (MPR) in a large in vitro fertilisation (IVF) programme before and after the introduction of single blastocyst transfer (SBT) strategy in a selected group of women.
Design: A 3-year pre- and postintervention study.
Setting: A tertiary reproductive medicine and assisted conception unit in a London teaching hospital.
Population: Two thousand four hundred and fifty-one fresh IVF cycles performed between July 2004 and June 2007 at the Assisted Conception Unit at Guy's and St Thomas' Hospital NHS Foundation Trust were included in the study.
Methods: In January 2006, we implemented a multidisciplinary intervention involving the introduction of a selective day 5 SBT service together with an educational programme on the risks of multiple pregnancy and potential advantages of blastocyst transfer aimed at couples at high risk of multiple pregnancy.
Main outcome measures: The CPR per cycle started and MPR per clinical pregnancy achieved.
Results: A statistically significant increase in the CPR from 27% (324/1198) to 32% (395/1253) (risk difference [RD] 5%, risk ratio [RR] 1.17, 95% CI 1.03-1.32, P= 0.015) and reduction in the MPR per clinical pregnancy from 32% (103/272) to 17% (69/395) (RD 15%, RR 0.46, 95% CI 0.35-0.60, P < 0.001) were observed after introduction of the SBT service.
Conclusion: Selective SBT in women with good prognosis can reduce the MPR after IVF while maintaining the overall success rate of the IVF programme.
Figures
References
-
- European Society Human Reproduction and Embryology. Assisted reproduction technology in Europe, 2000. Results generated from European registers by ESHRE. Hum Reprod. 2004;19:490–503. - PubMed
-
- HFEA register data 2003/2004. [1 June 2007]. www.hfea.gov.uk.
-
- El-Toukhy T, Khalaf Y, Braude P. IVF results: optimise not maximise. Am J Obstet Gynecol. 2006;194:322–31. - PubMed
-
- Walker M, Murphy K, Pan S, Yang Q, Wen S. Adverse maternal outcomes in multifetal pregnancies. BJOG. 2004;111:1294–6. - PubMed
-
- Pinborg A. IVF/ICSI twin pregnancies: risks and prevention. Hum Reprod Update. 2005;11:575–93. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
