

Improving patient adherence to lifestyle advice (IMPALA): a cluster-randomised controlled trial on the implementation of a nurse-led intervention for cardiovascular risk management in primary care (protocol)
- PMID: 18194522
- PMCID: PMC2267187
- DOI: 10.1186/1472-6963-8-9
Improving patient adherence to lifestyle advice (IMPALA): a cluster-randomised controlled trial on the implementation of a nurse-led intervention for cardiovascular risk management in primary care (protocol)
Abstract
Background: Many patients at high risk of cardiovascular diseases are managed and monitored in general practice. Recommendations for cardiovascular risk management, including lifestyle change, are clearly described in the Dutch national guideline. Although lifestyle interventions, such as advice on diet, physical exercise, smoking and alcohol, have moderate, but potentially relevant effects in these patients, adherence to lifestyle advice in general practice is not optimal. The IMPALA study intends to improve adherence to lifestyle advice by involving patients in decision making on cardiovascular prevention by nurse-led clinics. The aim of this paper is to describe the design and methods of a study to evaluate an intervention aimed at involving patients in cardiovascular risk management.
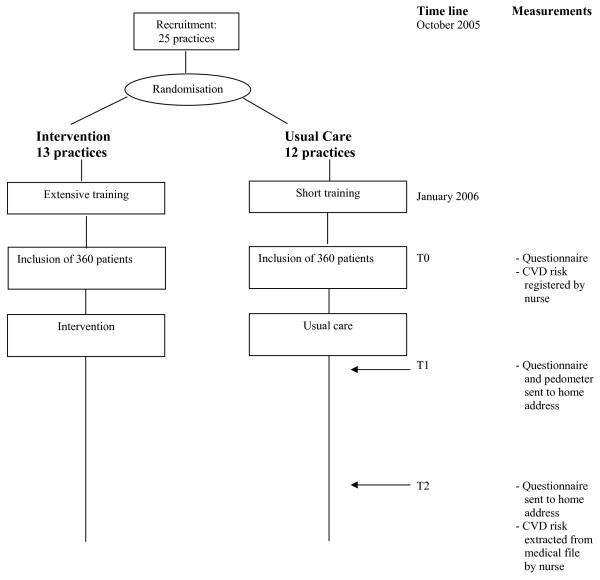
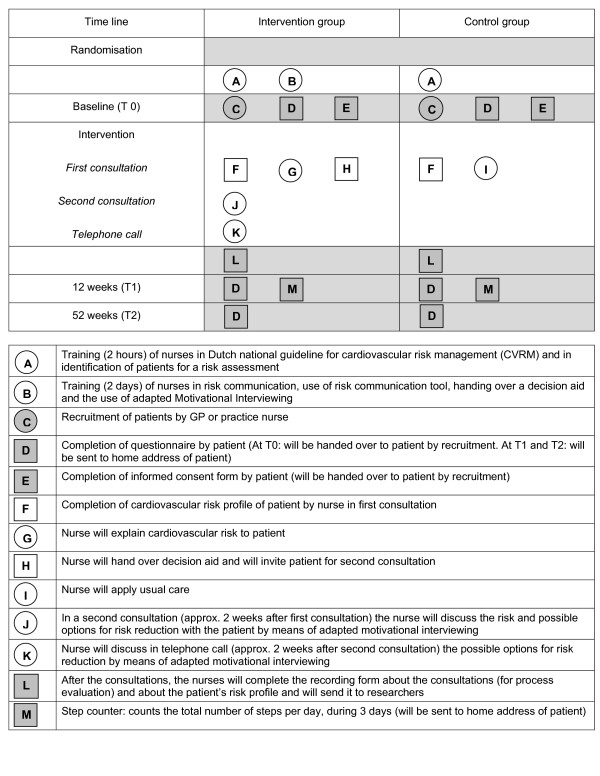
Methods: A cluster-randomised controlled trial in 20 general practices, 10 practices in the intervention arm and 10 in the control arm, starting on October 2005. A total of 720 patients without existing cardiovascular diseases but eligible for cardiovascular risk assessment will be recruited. In both arms, the general practitioners and nurses will be trained to apply the national guideline for cardiovascular risk management. Nurses in the intervention arm will receive an extended training in risk assessment, risk communication, the use of a decision aid and adapted motivational interviewing. This communication technique will be used to support the shared decision-making process about risk reduction. The intervention comprises 2 consultations and 1 follow-up telephone call. The nurses in the control arm will give usual care after the risk estimation, according to the national guideline. Primary outcome measures are self-reported adherence to lifestyle advice and drug treatment. Secondary outcome measures are the patients' perception of risk and their motivation to change their behaviour. The measurements will take place at baseline and after 12 and 52 weeks. Clinical endpoints will not be measured, but the absolute 10-year risk of cardiovascular events will be estimated for each patient from medical records at baseline and after 1 year.
Discussion: The combined use of risk communication, a decision aid and motivational interviewing to enhance patient involvement in decision making is an innovative aspect of the intervention.
Trial registration: Current Controlled Trials ISRCTN51556722.
Figures
References
-
- WHO . The World Health Report: conquering suffering, enriching humanity. Report of the Director-General. In: Organisation WH, editor. The World Health Report. Geneva , World Health Organisation; 1997.
-
- Koek HL, Engelfriet-Rijk CJM, Bots ML. Hart- en vaatziekten in Nederland. In: Jager-Geurts MH, Peters RJG, van Dis SJ, Bots ML, editor. Hart- en vaatziekten in Nederland 2006, cijfers over ziekte en sterfte. Den Haag , Nederlandse Hartstichting; 2006. pp. 9–21.
-
- WHO . The World Health Report: Reducing risks, promoting healthy lifestyle. . In: Organisation WH, editor. The World Health Report. Geneva , World Health Organisation; 2002.
-
- van Leest LATM, Verschuren WMM. Leeftstijl- en risicofactoren voor hart- en vaatziekten in de Nederlandse bevolking: prevalenties en trends. In: Jager-Geurts MH, Peters RJG, van Dis SJ, Bots ML, editor. Hart- en vaatziekten in Nederland 2006, cijfers over ziekte en sterfte. Den Haag , Nederlandse Hartstichting; 2006. pp. 89–107.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
