

doi: 10.1102/1470-7330/00/010077+09.
Modern surgery for liver metastases
Affiliations
- PMID: 18194890
- PMCID: PMC4554705
- DOI: 10.1102/1470-7330/00/010077+09
Item in Clipboard
Modern surgery for liver metastases
Cancer Imaging.
.
No abstract available
Figures
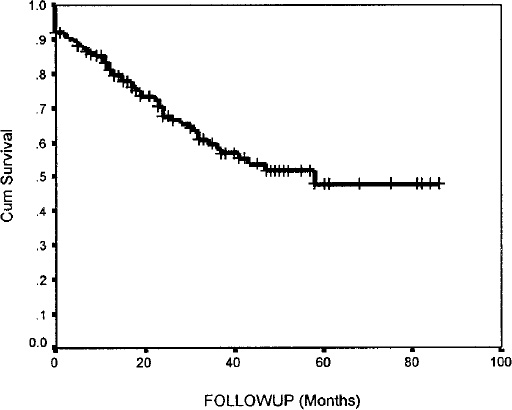
48% 5-year survival from hepatic resection (
n
=161).
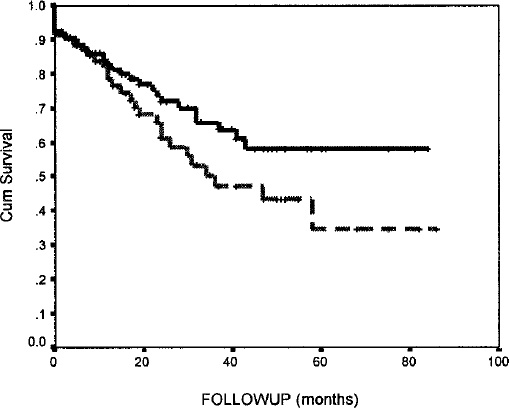
58% for bilateral resection (
n
=97); 35% for unilobar disease (
n
=64) at 5 years (
p
> 0.05). This demonstrates that patients with advanced disease can do well.
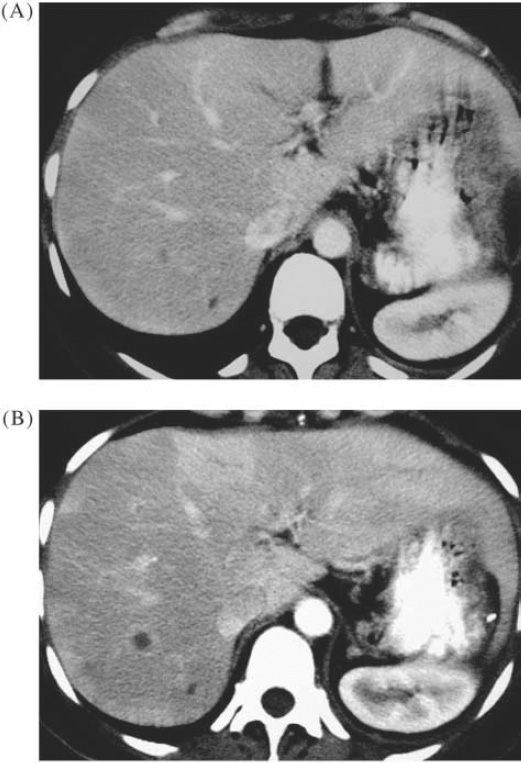
Metastasis from ovarian cancer. (A) CT showed lesions which are too small to characterize reliably; (B) CT 9 months later showed growth of metastasis.
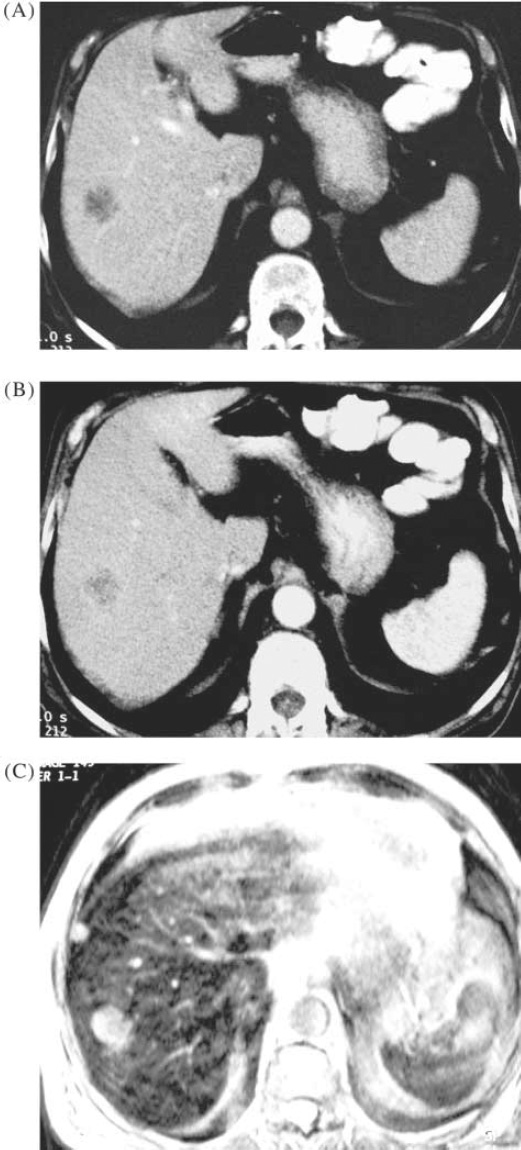
Colorectal metastases. Arterial phase CT (A) and portal phase CT (B) show a single metastasis. SPIO-enhanced MRI (C) shows an additional 1 cm lesion.
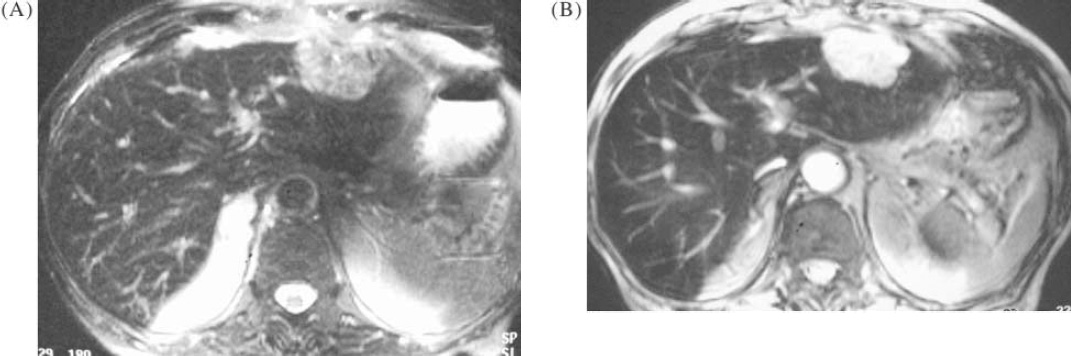
MR technique with SPIO. (A) T2-weighted FSE sequence shows large metastasis in left lobe; (B) optimized gradient echo T2 shows improved contrast between the tumour and normal liver, better visualization of vascular structures, and an additional lesion in segment 8.
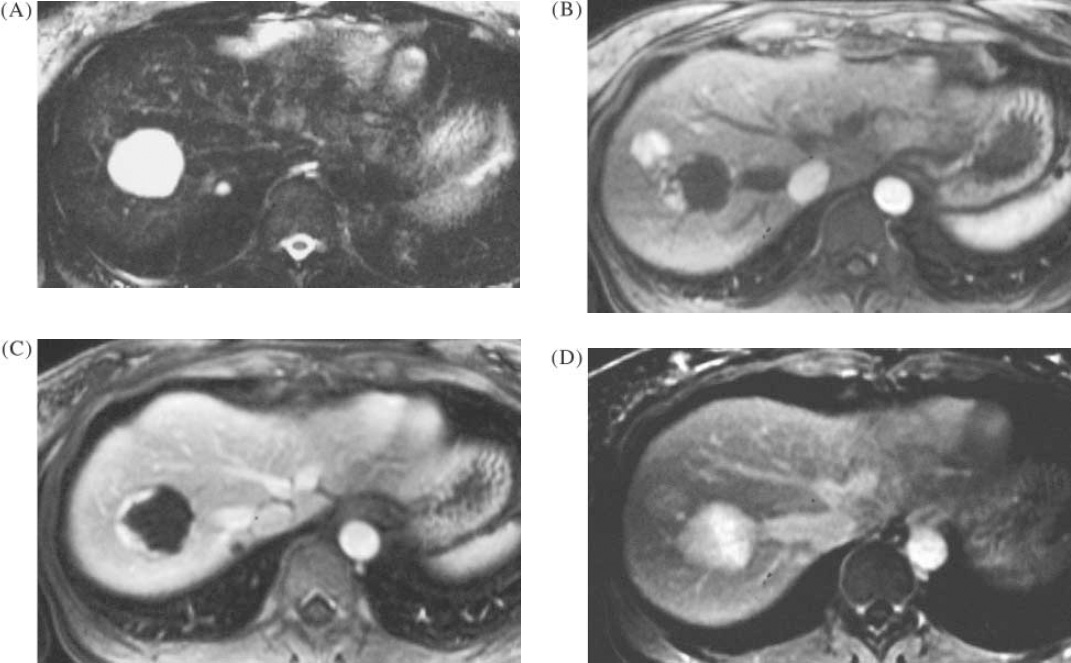
Benign liver lesions in a patient with colorectal cancer. (A) TSE T2 image showing 3 cm lesion which was indeterminate on ultrasound, also a second lesion of 7 mm. (B) and (C) T1-weighted image with gadolinium enhancement, arterial phases, showing typical peripheral nodular enhancement in the larger lesion but also an additional hypervascular lesion. Delayed post-gadolinium T1 image showing complete infilling of the 3 cm and 7 mm lesions, typical for haemangioma, and a faint persistent stain in the hypervascular lesion, suggestive of focal nodular hyperplasia. The FNH lesion was undetected on T2-weighted MRI, and also on ultrasound.
Similar articles
-
Factors determining the sensitivity of intraoperative ultrasonography in detecting colorectal liver metastases in the modern era.Ann Surg Oncol. 2010 Oct;17(10):2756-63. doi: 10.1245/s10434-010-1108-y. Epub 2010 Jun 2. Ann Surg Oncol. 2010. PMID: 20517682
-
[Surgical management of the colorectal carcinoma liver metastases].Rozhl Chir. 2009 Feb;88(2):69-74. Rozhl Chir. 2009. PMID: 19413263 Czech.
-
Adjuvant chemotherapy after resection of colorectal liver metastases in patients at high risk of hepatic recurrence: a comparative study between hepatic arterial infusion of oxaliplatin and modern systemic chemotherapy.Ann Surg. 2013 Jan;257(1):114-20. doi: 10.1097/SLA.0b013e31827b9005. Ann Surg. 2013. PMID: 23235397
-
Neoadjuvant treatment before resection of liver metastases.Eur J Surg Oncol. 2007 Dec;33 Suppl 2:S35-41. doi: 10.1016/j.ejso.2007.09.022. Epub 2007 Nov 5. Eur J Surg Oncol. 2007. PMID: 17981428 Review.
-
[Stereotactic body radiation therapy (SBRT) in the treatment of liver metastases: state of the art].Cancer Radiother. 2011 Feb;15(1):72-6. doi: 10.1016/j.canrad.2010.11.005. Epub 2011 Jan 8. Cancer Radiother. 2011. PMID: 21216647 Review. French.
Cited by
-
Magnetic resonance imaging of the liver: New imaging strategies for evaluating focal liver lesions.World J Radiol. 2009 Dec 31;1(1):72-85. doi: 10.4329/wjr.v1.i1.72. World J Radiol. 2009. PMID: 21160723 Free PMC article.
-
Liver metastases of colorectal cancer: US, CT or MR?Cancer Imaging. 2005 Nov 23;5 Spec No A(Spec No A):S149-56. doi: 10.1102/1470-7330.2005.0035. Cancer Imaging. 2005. PMID: 16361131 Free PMC article. Review.
-
Diagnostic performance of MDCT, PET/CT and gadoxetic acid (Primovist(®))-enhanced MRI in patients with colorectal liver metastases being considered for hepatic resection: initial experience in a single centre.Ir J Med Sci. 2012 Dec;181(4):499-509. doi: 10.1007/s11845-012-0805-x. Epub 2012 Mar 17. Ir J Med Sci. 2012. PMID: 22426901
-
Imaging diagnosis of colorectal liver metastases.World J Gastroenterol. 2011 Nov 14;17(42):4654-9. doi: 10.3748/wjg.v17.i42.4654. World J Gastroenterol. 2011. PMID: 22180707 Free PMC article. Review.
References
-
- Makuuchi M, Hasegawa H, Yamazaki S, Takayasu K. Four new hepatectomy procedures for resection of the right hepatic vein and preservation of the inferior right hepatic vein. Surg Gynecol Obstet. 1987;164:69–72. - PubMed
References
-
- Craig JR, Peters RL, Edmondson HA. Tumours of the liver and extrahepatic bile ducts. In: AFIP Atlas of tumour Pathology, Second series fascicle 26, 1989.
-
- Anthony SP, et al. Tumour and tumour-like lesions of the liver and biliary tract. In: MacSween RNM, et al., editors. Pathology of the Liver. 3. Edinburgh: Churchill Livingstone; 1994. pp. 635–711.
-
- Mytiroglou P, Theise ND. Differential diagnosis of hepatocellular nodular lesions. Semin Diagn Pathol. 1998;15:285–99. - PubMed
References
-
- Blomley M, Cosgrove D. Contrast agents in ultrasound. Br J Hosp Med. 1996;55:6–7. - PubMed
-
- Leen E, McArdle CS. Ultrasound contrast agents in liver imaging. Clin Radiol. 1996;51(Suppl1):35–9. - PubMed
-
- Eckersley R. Functional Imaging with ultrasound contrast agents. Ultrasound Med Biol 1999 (in press).
References
-
- Willis RA. The spread of Tumours in the Human Body. 3. London: Butterworths; 1973. Secondary tumours of the liver; pp. 175–83.
-
- Ozarda A, Pickren J. The topographic distribution of liver metastases, its relation to surgical and isotope diagnosis. J Nucl Med. 1962;3:149–52.
LinkOut - more resources
Full Text Sources