

Explaining patients' beliefs about the necessity and harmfulness of antidepressants
- PMID: 18195311
- PMCID: PMC2203394
- DOI: 10.1370/afm.759
Explaining patients' beliefs about the necessity and harmfulness of antidepressants
Abstract
Purpose: Patients' beliefs about antidepressants vary widely and probably influence adherence, yet little is known about what underlies such beliefs. This study's objective was to identify the demographic and clinical characteristics that account for patients' beliefs about antidepressants.
Methods: Participants were 165 patients with unipolar nonpsychotic major depression from primary care and psychiatry clinics who were participating in the baseline phase of a multistaged trial of medication and psychotherapy. Before patients started antidepressants, interview and self-report measures were used to assess treatment beliefs, depression features, and comorbid conditions. Linear multivariate regression was used to identify the strongest correlates of perceived medication necessity and harmfulness after adjusting for age, sex, education, and the random effects of patients within clinical site.
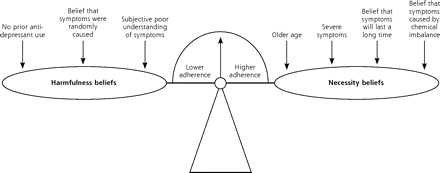
Results: Perceived necessity was associated with older age (P <.001), more severe symptoms (P = .03), longer anticipated duration of symptoms (P=.001), and attribution of symptoms to chemical imbalance (P=.005). Perceived harmfulness was highest among patients who had not taken antidepressants before (P = .02), attributed their symptoms to random factors (P=.04), and had a subjectively unclear understanding of depression (P = .003). Neither belief was significantly associated with sex, education, age at first depressive episode, presence of melancholia or anxiety, psychiatric comorbidity, or clinical setting.
Conclusions: Skepticism about antidepressants is strongest among younger patients who have never taken antidepressants, view their symptoms as mild and transient, and feel unclear about the factors affecting their depression. Perhaps these patients would benefit the most from adherence promotion focusing on treatment beliefs.
Figures
References
-
- Depression Guideline Panel. Depression in Primary Care: Volume 1. Detection and Diagnosis. Clinical Practice Guideline, Number 5. Rockville, MD: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1993. AHCPR publication 93–0550.
-
- Maixner SM, Greden JF. Extended antidepressant maintenance and discontinuation syndromes. Depress Anxiety. 1998;8(Suppl 1):43–53. - PubMed
-
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry. 2000;157(4 Suppl):1–45. - PubMed
-
- Lin E, Von Korff M, Katon W, et al. The role of the primary care physician in patients’ therapy. Med Care. 1995;33(1):67–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources