

Breast metastasis from small cell lung carcinoma
- PMID: 18196611
- PMCID: PMC2170467
- DOI: 10.1631/jzus.B072258
Breast metastasis from small cell lung carcinoma
Abstract
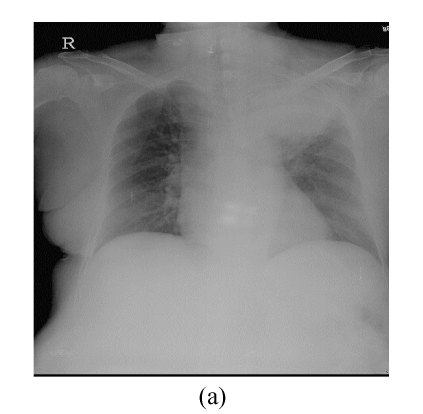
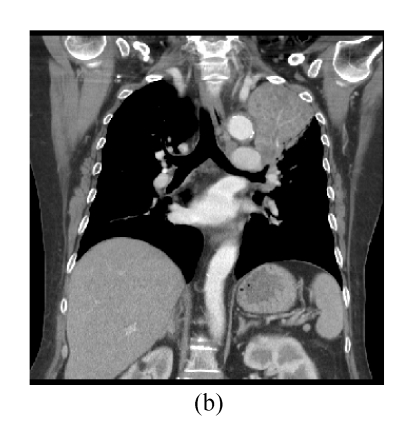
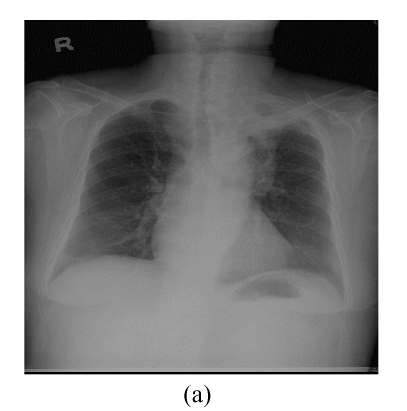
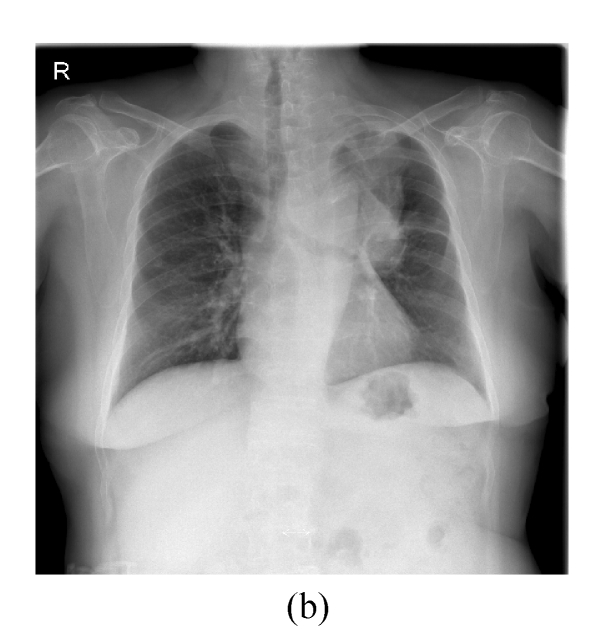
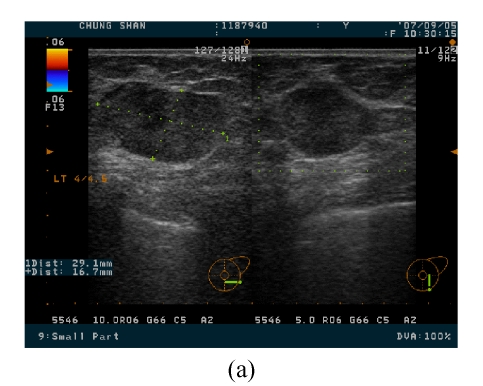
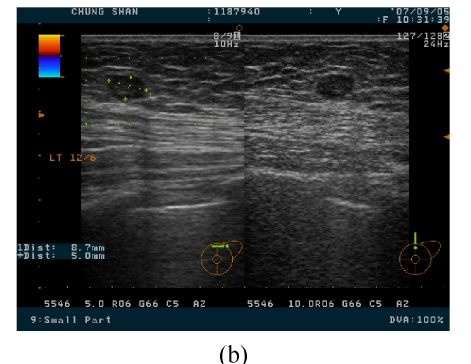
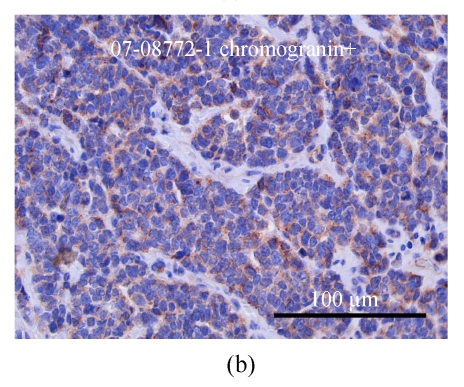
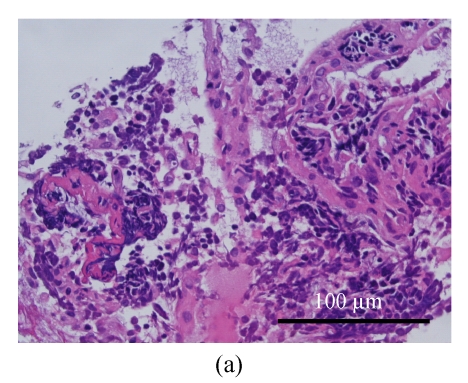
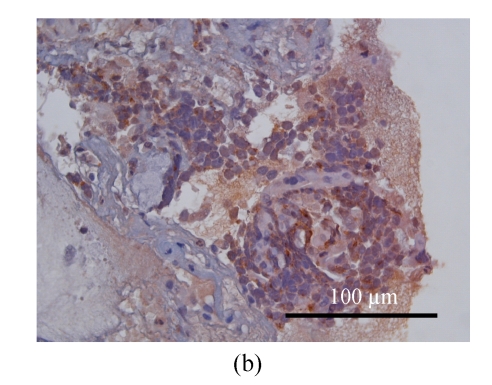
Breast metastases from extramammary neoplasms are very rare. We presented a 66 year-old female with metastasis of small cell lung carcinoma to the breast. She presented with consolidation over the left upper lobe of her lung undetermined after endobronchial or video-assisted thoracoscopic surgery (VATS) biopsy, and this was treated effectively after antibiotic therapy at initial stage. The left breast lumps were noted 4 months later, and she underwent a modified radical mastectomy under the impression of primary breast carcinoma. However, the subsequent chest imaging revealed re-growing mass over the left mediastinum and hilum, and cells with the same morphological and staining features were found from specimens of transbronchial brushing and biopsy. An accurate diagnosis to distinguish a primary breast carcinoma from metastatic one is very important because the therapeutic planning and the outcome between them are different.
Figures
Similar articles
-
[A case of small cell lung cancer with an initial symptom of breast metastasis].Nihon Kokyuki Gakkai Zasshi. 2006 Jan;44(1):39-42. Nihon Kokyuki Gakkai Zasshi. 2006. PMID: 16502865 Japanese.
-
Squamous cell lung carcinoma metastatic to the breast.Anticancer Res. 2008 Mar-Apr;28(2B):1299-301. Anticancer Res. 2008. PMID: 18505069
-
Metastasis to the breast from an adenocarcinoma of the lung with extensive micropapillary component: a case report and review of the literature.Diagn Pathol. 2010 Dec 17;5:82. doi: 10.1186/1746-1596-5-82. Diagn Pathol. 2010. PMID: 21167048 Free PMC article. Review.
-
Diagnosis and natural history of extramammary tumors metastatic to the breast.J Am Coll Surg. 1995 Mar;180(3):381-2. J Am Coll Surg. 1995. PMID: 7874353 No abstract available.
-
Breast lumps: rare presentation of oat cell carcinoma of lung.J Clin Pathol. 1988 Feb;41(2):171-2. doi: 10.1136/jcp.41.2.171. J Clin Pathol. 1988. PMID: 2832451 Free PMC article. Review.
Cited by
-
Lung cancer masquerading as breast cancer with carcinoma en cuirasse.BMJ Case Rep. 2014 Nov 13;2014:bcr2014206596. doi: 10.1136/bcr-2014-206596. BMJ Case Rep. 2014. PMID: 25395467 Free PMC article.
-
A Rare Case of Breast Metastasis from a Primary Lung Tumor: Case Report.Curr Oncol. 2024 Aug 16;31(8):4695-4703. doi: 10.3390/curroncol31080350. Curr Oncol. 2024. PMID: 39195333 Free PMC article.
-
Bilateral breast lumps as a presentation of disseminated squamous cell carcinoma of lung.Clin Med Insights Case Rep. 2014 Feb 18;7:21-3. doi: 10.4137/CCRep.S13832. eCollection 2014. Clin Med Insights Case Rep. 2014. PMID: 24653651 Free PMC article.
-
Uncommon Tumors and Uncommon Presentations of Cancer in the Breast.Curr Breast Cancer Rep. 2021 Nov 1;13(4):331-346. doi: 10.1007/s12609-021-00435-x. Curr Breast Cancer Rep. 2021. PMID: 36589040 Free PMC article.
-
Breast metastases from primary lung cancer: a retrospective case series on clinical, ultrasonographic, and immunohistochemical features.Transl Lung Cancer Res. 2021 Jul;10(7):3226-3235. doi: 10.21037/tlcr-21-542. Transl Lung Cancer Res. 2021. PMID: 34430360 Free PMC article.
References
-
- Cangiarella J, Symmans WF, Cohen JM, Goldenberg A, Shapiro RL, Waisman J. Malignant melanoma metastatic to the breast: a report of seven cases diagnosed by fine-needle aspiration cytology. Cancer. 1998;84(3):160–162. doi: 10.1002/(SICI)1097-0142(19980625)84:3<160::AID-CNCR7>3.0.CO;2-S. - DOI - PubMed
-
- Chaignaud B, Hall TJ, Powers C, Subramony C, Scott-Conner CE. Diagnosis and natural history of extramammary tumors metastatic to the breast. J Am Coll Surg. 1994;179(1):49–53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
