

Effects of plasma expansion with albumin and paracentesis on haemodynamics and kidney function in critically ill cirrhotic patients with tense ascites and hepatorenal syndrome: a prospective uncontrolled trial
- PMID: 18197961
- PMCID: PMC2374626
- DOI: 10.1186/cc6765
Effects of plasma expansion with albumin and paracentesis on haemodynamics and kidney function in critically ill cirrhotic patients with tense ascites and hepatorenal syndrome: a prospective uncontrolled trial
Abstract
Introduction: Circulatory dysfunction in cirrhotic patients may cause a specific kind of functional renal failure termed hepato-renal syndrome (HRS). It contributes to the high incidence of renal failure in cirrhotic intensive care unit (ICU) patients. Fluid therapy may aggravate renal failure by increasing ascites and intra-abdominal pressure (IAP). This study investigates the short-term effects of paracentesis on haemodynamics and kidney function in volume resuscitated patients with HRS.
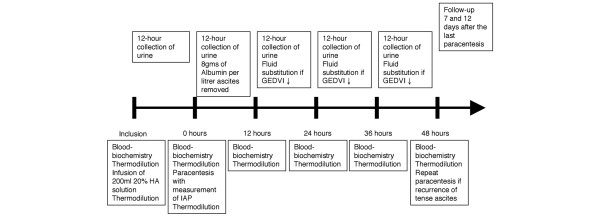
Methods: Nineteen consecutive cirrhotic patients with HRS were studied. Circulatory parameters and renal function were analysed before and after plasma expansion and paracentesis. Haemodynamic monitoring was performed by transpulmonary thermodilution.
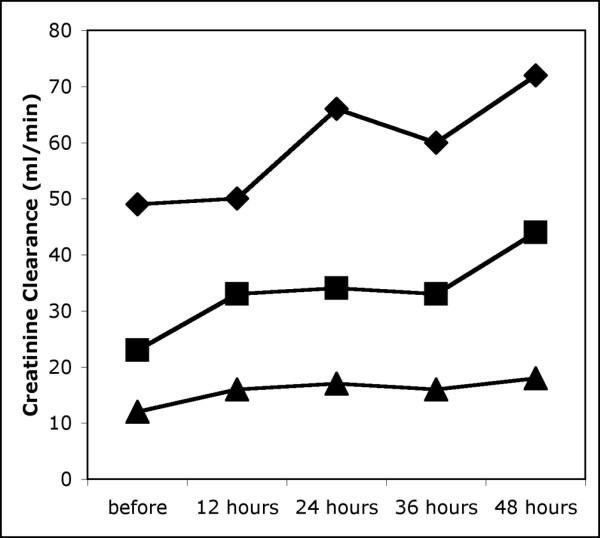
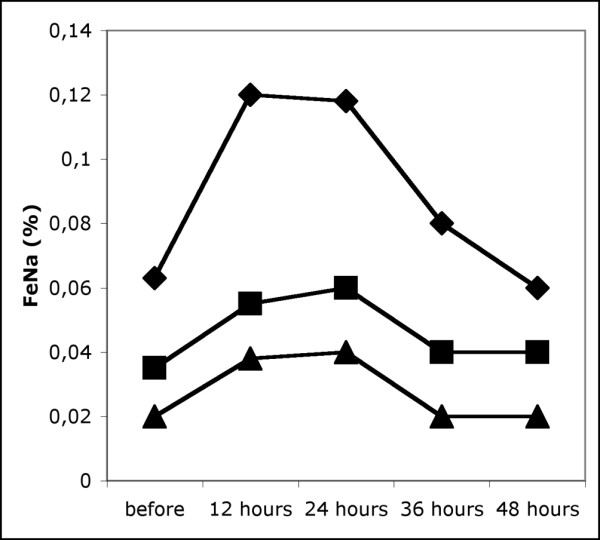
Results: After infusion of 200 ml of 20% human albumin solution, mean arterial pressure (MAP) and central venous pressure remained unchanged. Global end-diastolic volume index (GEDVI) increased from 791 ml m(-2) (693 to 862) (median and 25th to 75th percentile) to 844 ml m(-2) (751 to 933). Cardiac index (CI) increased from 4.1 l min(-1) m(-2) (3.6 to 5.0) to 4.7 l min(-1) m(-2) (4.0 to 5.8), whereas systemic vascular resistance index (SVRI) decreased from 1,422 dyn s cm(-5) m(-2) (1,081 to 1,772) to 1,171 dyn s cm(-5) m(-2) (893 to 1,705). Creatinine clearance (CC) and fractional excretion of sodium (FeNa) were not affected. During paracentesis, IAP decreased from 22 mmHg (18 to 24) to 9 mmHg (8 to 12). MAP decreased from 81 mmHg (74 to 100) to 80 mmHg (71 to 89), and CI increased from 4.1 l min(-1) m(-2) (3.2 to 4.3) to 4.2 l min(-1) m(-2) (3.6 to 4.7), whereas SVRI decreased from 1,639 dyn s cm(-5) m(-2) (1,168 to 2,037) to 1,301 dyn s cm(-5) m(-2) (1,124 to 1,751). CC during the 12-hour interval after paracentesis was significantly higher than during the 12 hours before (33 ml min(-1) (16 to 50) compared with 23 ml min(-1) (12 to 49)). CC remained elevated for the rest of the observation period. FeNa increased after paracentesis but returned to baseline levels after 24 hours.
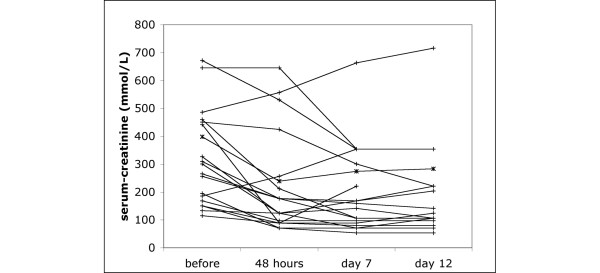
Conclusion: Paracentesis with parameter-guided fluid substitution and maintenance of central blood volume may improve renal function and is safe in the treatment of ICU patients with hepato-renal failure.
Figures
Comment in
-
Towards goal-directed therapy of hepatorenal syndrome: we have the tools but we need the trials.Crit Care. 2008;12(2):119. doi: 10.1186/cc6804. Epub 2008 Mar 19. Crit Care. 2008. PMID: 18394181 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
