

Diagnostic performance of an expert system for interpretation of 99mTc MAG3 scans in suspected renal obstruction
- PMID: 18199609
- PMCID: PMC3179983
- DOI: 10.2967/jnumed.107.045484
Diagnostic performance of an expert system for interpretation of 99mTc MAG3 scans in suspected renal obstruction
Abstract
The purpose of the study was to compare diuresis renography scan interpretation generated by a renal expert system with the consensus interpretation of 3 expert readers.
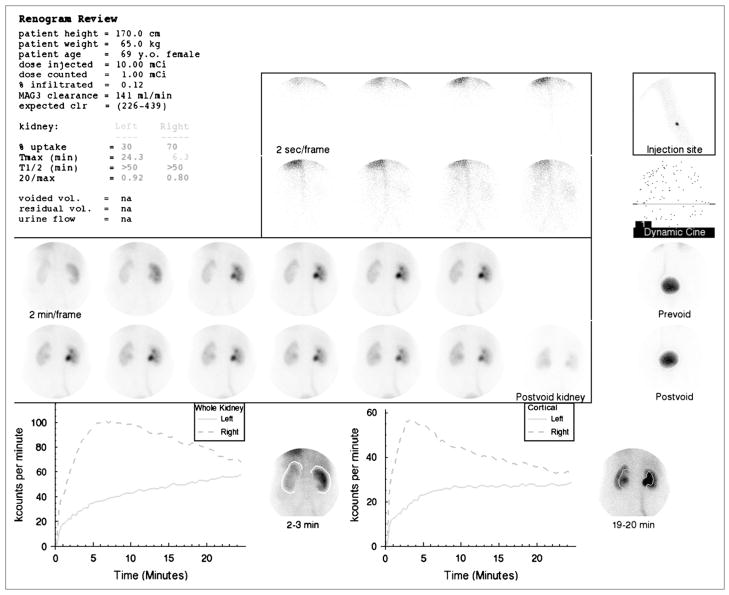
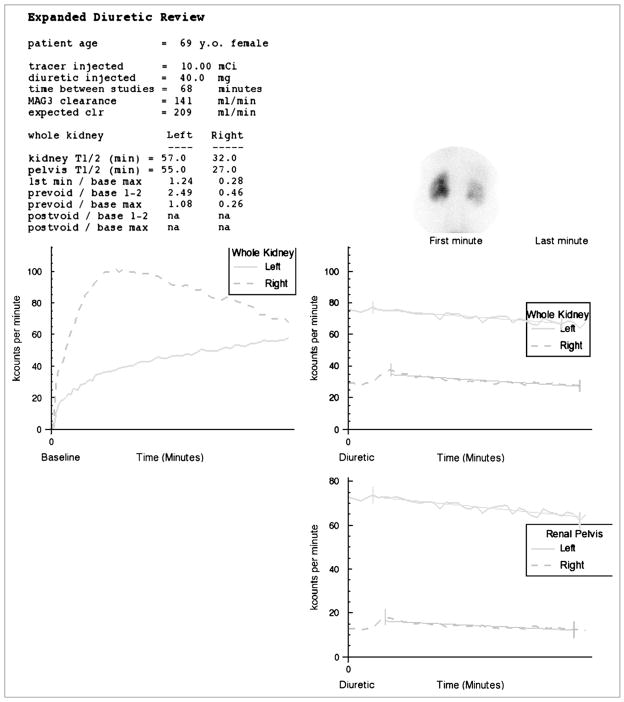
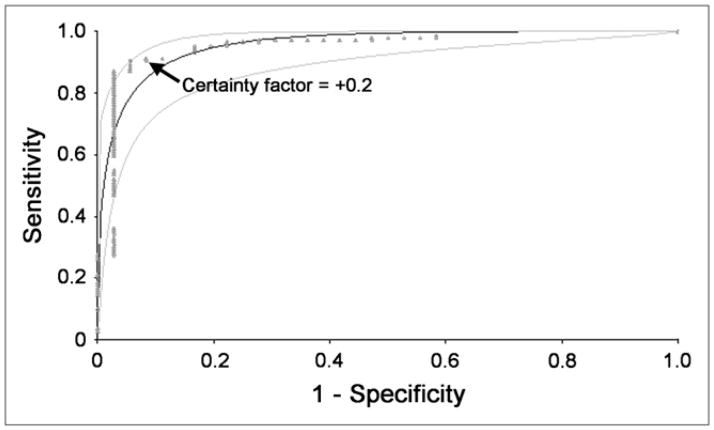
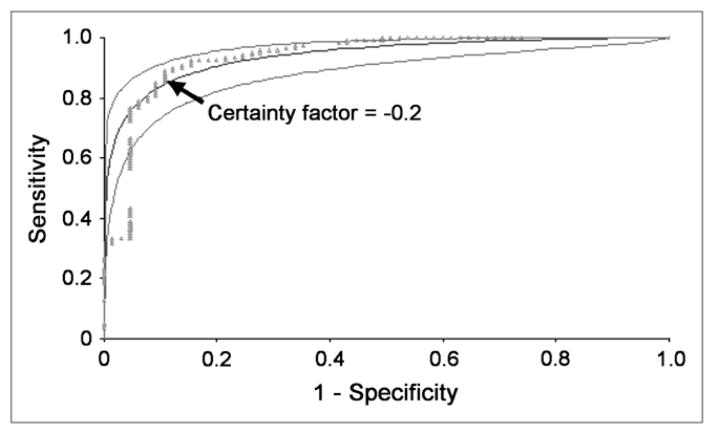
Methods: The expert system was evaluated in 95 randomly selected furosemide-augmented patient studies (185 kidneys) obtained for suspected obstruction; there were 55 males and 40 females with a mean age +/- SD of 58.6 +/- 16.5 y. Each subject had a baseline (99m)Tc-mercaptoacetyltriglycine ((99m)Tc-MAG3) scan followed by furosemide administration and a separate 20-min acquisition. Quantitative parameters were automatically extracted from baseline and furosemide acquisitions and forwarded to the expert system for analysis. Three experts, unaware of clinical information, independently graded each kidney as obstructed/probably obstructed, equivocal, and probably nonobstructed/nonobstructed; experts resolved differences by a consensus reading. These 3 expert categories were compared with the obstructed, equivocal, and nonobstructed interpretations provided by the expert system. Agreement was assessed using weighted kappa, and the predictive accuracy of the expert system compared with expert readers was assessed by the area under receiver-operating-characteristic (ROC curve) curves.
Results: The expert system agreed with the consensus reading in 84% (101/120) of nonobstructed kidneys, in 92% (33/36) of obstructed kidneys, and in 45% (13/29) of equivocal kidneys. The weighted kappa between the expert system and the consensus reading was 0.72 and was comparable with the weighted kappa between experts. There was no significant difference in the areas under the ROC curves when the expert system was compared with each expert using the other 2 experts as the gold standard.
Conclusion: The renal expert system showed good agreement with the expert interpretation and could be a useful educational and decision support tool to assist physicians in the diagnosis of renal obstruction. To better mirror the clinical setting, algorithms to incorporate clinical data must be designed, implemented, and tested.
Conflict of interest statement
The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict-of-interest practice.
Figures
References
-
- O’Reilly P, Aurell M, Britton K, Kletter K, Rosenthal L, Testa T. Consensus on diuresis renography for investigating the dilated upper urinary tract. J Nucl Med. 1996;37:1872–1876. - PubMed
-
- IMV Medical Information Division. 2003 Nuclear Medicine Census Marke Summary Report. IV. Des Plaines, IL: IMV, Ltd; 2003. pp. 7–11.
-
- Garcia EV, Taylor A, Halkar R, et al. RENEX: an expert system for the interpretation of 99mTc-MAG3 scans to detect renal obstruction. J Nucl Med. 2006;47:320–329. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources