

Assessment of racial disparities in chronic kidney disease stage 3 and 4 care in the department of defense health system
- PMID: 18199843
- PMCID: PMC2390939
- DOI: 10.2215/CJN.03940907
Assessment of racial disparities in chronic kidney disease stage 3 and 4 care in the department of defense health system
Abstract
Background and objectives: Racial disparities in provision of healthcare are widespread in the United States but have not been specifically assessed in provision of chronic kidney disease (CKD) care.
Design, setting, participants, & measurements: We conducted a retrospective cohort study of the clinical database used in a Department of Defense (DOD) medical system. Beneficiaries studied were DOD-eligible beneficiaries with CKD stage 3 (n = 7729) and 4 (n = 589) using the modified Modification of Diet in Renal Disease (MDRD)-estimated GFR formula but requiring manual correction for Black race. Compliance with selected Kidney Disease Outcomes Quality Initiative (KDOQI) CKD recommended targets (monitoring of recommended laboratory data, prescription of recommended medications, and referral to nephrology) was assessed over a 12-mo period, stratified by CKD stage. Logistic regression analysis was used to assess whether race (White, Black, or other) was independently associated with provider compliance with targets, adjusted for demographic factors and burden of comorbid conditions.
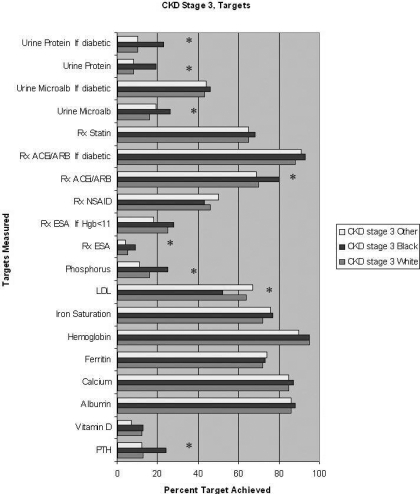
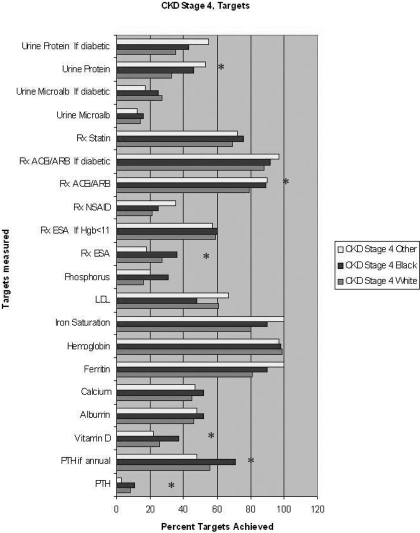
Results: Among the targets, only monitoring of LDL cholesterol was significantly less common among Blacks. For all other measures, compliance was either not significantly different or significantly higher for Black compared with White beneficiaries. However, patients categorized as "Other" race were in general less likely to achieve targets than Whites, and at stage 3 CKD significantly less likely to achieve targets for monitoring of phosphorous, hemoglobin, and vitamin D.
Conclusions: In the DOD health system, provider compliance with selected CKD stage 3 and 4 targets was not significantly lower for Black beneficiaries than for Whites, with the exception of LDL cholesterol monitoring. Patients classified as Other race were generally less likely to achieve targets than Whites, in some patients significantly so.
Figures
Comment in
-
Racial disparities in chronic kidney disease: tragedy, opportunity, or both?Clin J Am Soc Nephrol. 2008 Mar;3(2):314-6. doi: 10.2215/CJN.00370108. Epub 2008 Feb 20. Clin J Am Soc Nephrol. 2008. PMID: 18287256 Free PMC article. No abstract available.
References
-
- Popescu I, Vaughan-Sarrazin MS, Rosenthal GE: Differences in mortality and use of revascularization in Black and White beneficiaries with acute MI admitted to hospitals with and without revascularization services. JAMA 297: 2489–2495, 2007 - PubMed
-
- Satcher D, Fryer GE, McCann J, Troutman A, Woolf SH, Rust G: What if we were equal? A comparison of the Black-White mortality gap in 1960 and 2000. Health Affairs 24: 459–465, 2005 - PubMed
-
- Eckhoff DE, Young CJ, Gaston RS, Fineman SW, Deierhoi MH, Foushee MT, Brown RN, Diethelm AG: Racial disparities in renal allograft survival: A public health issue? J Am Coll Surg 204: 894–902, 2007 - PubMed
-
- McClellan W, Warnock DG, McClure L, Campbell RC, Newsome BB, Howard V, Cushman M, Howard G: Racial differences in the prevalence of chronic kidney disease among participants in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) Cohort Study. J Am Soc Nephrol 17: 1710–1715, 2006 - PubMed
-
- Garg PP, Diener-West M, Powe NR: Reducing racial disparities in transplant activation: Whom should we target? Am J Kidney Dis 37: 921–931, 2001 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
