

Primary sclerosing cholangitis, autoimmune hepatitis and overlap syndromes in inflammatory bowel disease
- PMID: 18200656
- PMCID: PMC2679122
- DOI: 10.3748/wjg.14.331
Primary sclerosing cholangitis, autoimmune hepatitis and overlap syndromes in inflammatory bowel disease
Abstract
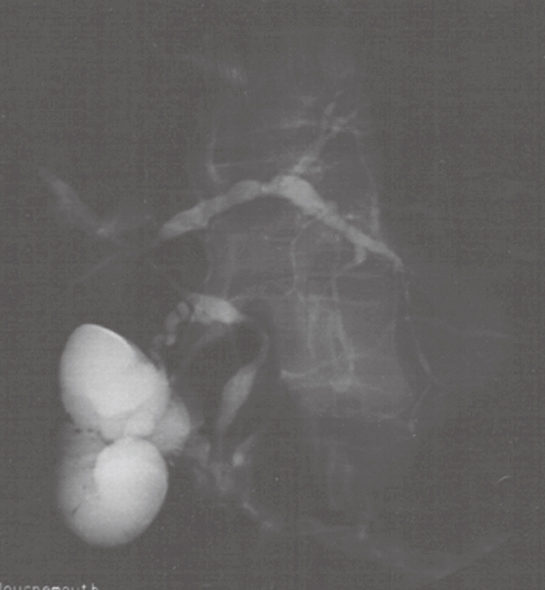
Primary sclerosing cholangitis (PSC) is a chronic progressive disorder of unknown aetiology characterised by chronic inflammation and stricture formation of the biliary tree. Symptoms include itch and lethargy and in advanced cases cholangitis and end-stage liver disease, however increasing numbers of asymptomatic individuals are being identified. The disease is rare in the general population but is strongly associated with inflammatory bowel disease (IBD) affecting up to 5% of patients with ulcerative colitis, with a slightly lower prevalence (up to 3.6%) in Crohn's disease. The strength of this association means that the vast majority (> 90%) of patients with PSC also have IBD, although many may have only mild gastro-intestinal symptoms. Usually IBD presents before PSC, although vice-versa can occur and the onset of both conditions can be separated in some cases by many years. Mean age of diagnosis of PSC is in the fifth decade of life with a strong male predominance. Risk is increased in those with a family history of PSC, suggesting a genetic predisposition and the disease is almost exclusive to non-smokers. The ulcerative colitis associated with PSC is characteristically mild, runs a quiescent course, is associated with rectal sparing, more severe right sided disease, backwash ileitis and has a high risk of pouchitis post-colectomy. Most worrisome is the high risk of colorectal malignancy which necessitates routine colonoscopic surveillance. Cholangiocarcinoma is also a frequent complication of PSC with a 10%-15% lifetime risk of developing this condition. Treatment with high dose ursodeoxycholic acid offers some chemoprotective effects against colorectal malignancy and may decrease symptoms, biochemical and histological progression of liver disease. Small duct PSC patients characteristically have normal cholangiography, and liver biopsy is required for diagnosis, it appears to have a more favourable prognosis. Autoimmune Hepatitis (AIH) is also more prevalent in patients with IBD, with up to 16% of patients with AIH also having ulcerative colitis. A small subgroup of patients have a AIH-PSC overlap syndrome and the management of these patients depends on liver histology, serum IgM levels, autoantibodies, degree of biochemical cholestasis and cholangiography as some of these patients may respond to immunosuppression.
Figures
References
-
- Thomas CH. Ulceration of the colon with a much enlarged fatty liver. Trans Pathol Soc Phil. 1873;4:87–88.
-
- Lister JD. A specimen of diffuse ulcerative colitis with secondary diffuse hepatitis. Trans Pathol Soc Lon. 1899;50:130–134.
-
- Smith MP, Loe RH. Sclerosing cholangitis; review of recent case reports and associated diseases and four new cases. Am J Surg. 1965;110:239–246. - PubMed
-
- Lee YM, Kaplan MM. Primary sclerosing cholangitis. N Engl J Med. 1995;332:924–933. - PubMed
-
- Angulo P, Lindor KD. Primary sclerosing cholangitis. Hepatology. 1999;30:325–332. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
