

Comparison of self-administered vaginal misoprostol versus placebo for cervical ripening prior to operative hysteroscopy using a sequential trial design
- PMID: 18201279
- PMCID: PMC2345467
- DOI: 10.1111/j.1471-0528.2007.01628.x
Comparison of self-administered vaginal misoprostol versus placebo for cervical ripening prior to operative hysteroscopy using a sequential trial design
Abstract
Objective: To compare the impact of 1000 micrograms of self-administered vaginal misoprostol versus self-administered vaginal placebo at home on preoperative cervical ripening in both premenopausal and postmenopausal women before operative hysteroscopy.
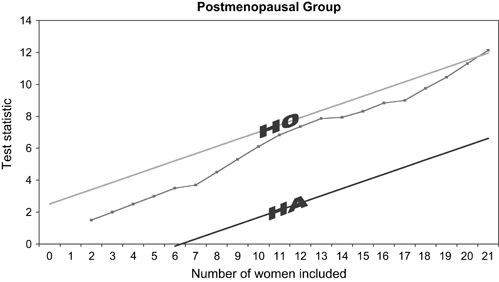
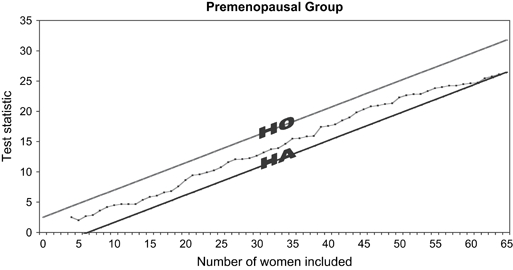
Design: Two separate but identical parallel, randomised, double-blind, placebo-controlled sequential trials, one in premenopausal women and one in postmenopausal women. The boundaries for the sequential trials were calculated on the primary outcomes of a difference of cervical dilatation > or = 1 mm, with the assumption of a type 1 error of 0.05 and a power of 0.95.
Setting: Norwegian university teaching hospital.
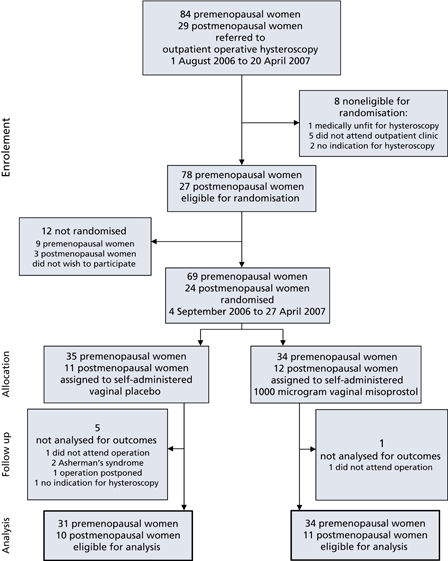
Sample: Eighty-six women referred to outpatient operative hysteroscopy.
Methods: The women were randomised to either 1000 micrograms of self-administered vaginal misoprostol or self-administered vaginal placebo the evening before outpatient operative hysteroscopy.
Main outcome measures: Preoperative cervical dilatation (primary outcome), number of women who achieve a preoperative cervical dilatation > or = 5 mm, acceptability, complications and adverse effects (secondary outcomes).
Results: In premenopausal women, the mean cervical dilatation was 6.4 mm (SD 2.4) in the misoprostol group and 4.8 mm (SD 2.0) in the placebo group, the mean difference in cervical dilatation being 1.6 mm (95% CI 0.5-2.7). Among the premenopausal women receiving misoprostol, 88% achieved a cervical dilatation of > or = 5 mm compared with 65% in the placebo group. Twelve percent of the women who received misoprostol were difficult to dilate compared with 32% who received placebo. Dilatation was also quicker in the misoprostol group. Misoprostol had no effect on cervical ripening in postmenopausal women compared with placebo, and 43% of the women were difficult to dilate. The trials were terminated after analysis of 21 postmenopausal women and 65 premenopausal women after reaching a conclusion on the primary outcome with only 28% of the number of women needed in a fixed sample size trial. Three of 45 women who received misoprostol experienced severe lower abdominal pain, and there was an increased occurrence of light preoperative bleeding in the misoprostol group. Most women did not experience misoprostol-related adverse effects. The majority (83% of premenopausal and 76% of postmenopausal women) found self-administered vaginal misoprostol at home to be acceptable. There were two serious complications in the premenopausal misoprostol group: uterine perforation with subsequent peritonitis and heavy postoperative bleeding requiring blood transfusion, but these were not judged to be misoprostol related. Complications were otherwise comparatively minor and distributed equally between the two dosage groups.
Conclusions: One thousand micrograms of self-administered vaginal misoprostol 12 hours prior to operative hysteroscopy has a significant cervical ripening effect compared with placebo in premenopausal but not in postmenopausal women. Self-administered vaginal misoprostol of 1000 micrograms at home the evening before operative hysteroscopy is safe and highly acceptable, although a small proportion of women experienced severe lower abdominal pain. There is a risk of lower abdominal pain and light preoperative bleeding with this regimen, which is very cheap and easy to use.
Figures
Comment in
-
Comparison of self-administered vaginal misoprostol versus placebo for cervical ripening prior to operative hysteroscopy using a sequential trial design.BJOG. 2008 Aug;115(9):1188; author reply 1189. doi: 10.1111/j.1471-0528.2008.01818.x. BJOG. 2008. PMID: 18715444 No abstract available.
-
Comparison of self-administered vaginal misoprostol versus placebo for cervical ripening prior to operative hysteroscopy using a sequential trial design.BJOG. 2008 Aug;115(9):1188-9; author reply 1189. doi: 10.1111/j.1471-0528.2008.01815.x. BJOG. 2008. PMID: 18715446 No abstract available.
-
Vaginal misoprostol for cervical ripening prior to hysteroscopy.BJOG. 2008 Dec;115(13):1720; author reply 1720-1. doi: 10.1111/j.1471-0528.2008.01909.x. BJOG. 2008. PMID: 19035958 No abstract available.
References
-
- Marjoribanks J, Lethaby A, Farquhar C. Surgery versus medical therapy for heavy menstrual bleeding (Cochrane review) Cochrane Database Syst Rev. 2006 CD003855. - PubMed
-
- Bradley LD. Complications in hysteroscopy: prevention, treatment and legal risk. Curr Opin Obstet Gynecol. 2002;14:409–15. - PubMed
-
- Lieng M, Qvigstad E, Sandvik L, Jørgensen H, Langebrekke A, Istre O. Hysteroscopic resection of symptomatic and asymptomatic endometrial polyps. J Minim Invasive Gynecol. 2007;14:189–94. - PubMed
-
- Grimes DA, Schulz KF, Cates WJ., Jr Prevention of uterine perforation during curettage abortion. JAMA. 1984;251:2108–11. - PubMed
-
- Schulz KF, Grimes DA, Cates W. Measures to prevent cervical injury during suction curettage abortion. Lancet. 1983;1:1182–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
