

Effects of pathologic stage on the learning curve for radical prostatectomy: evidence that recurrence in organ-confined cancer is largely related to inadequate surgical technique
- PMID: 18207316
- PMCID: PMC2637145
- DOI: 10.1016/j.eururo.2008.01.005
Effects of pathologic stage on the learning curve for radical prostatectomy: evidence that recurrence in organ-confined cancer is largely related to inadequate surgical technique
Abstract
Objectives: We previously demonstrated that there is a learning curve for open radical prostatectomy. We sought to determine whether the effects of the learning curve are modified by pathologic stage.
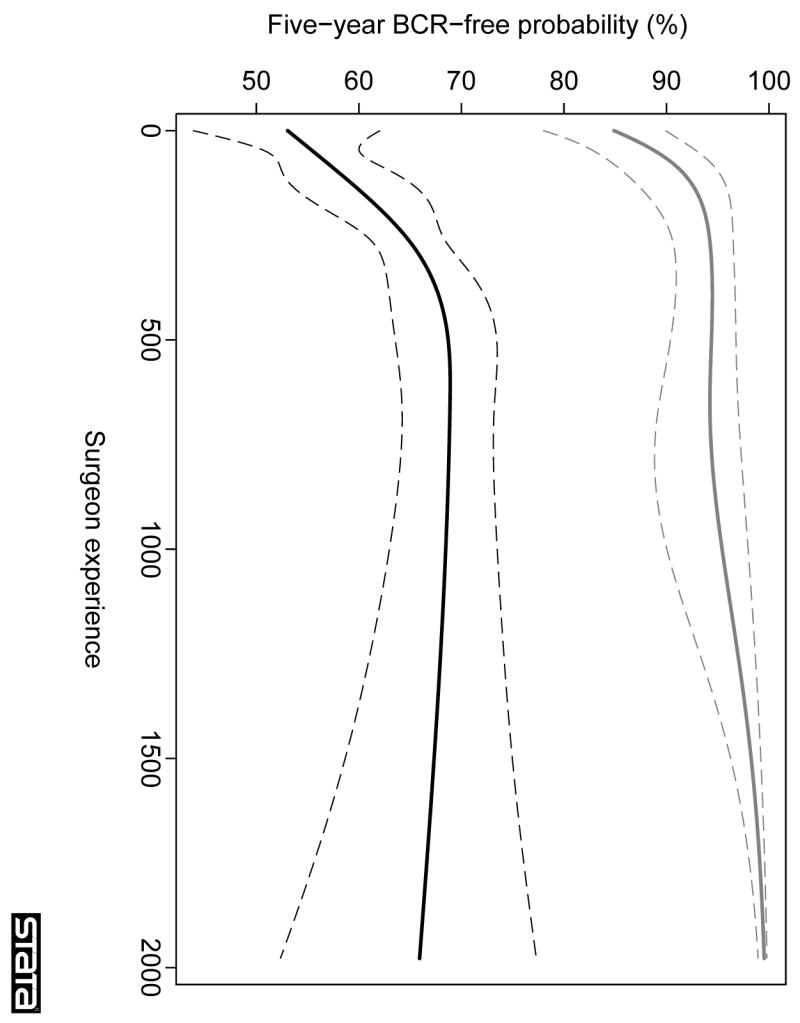
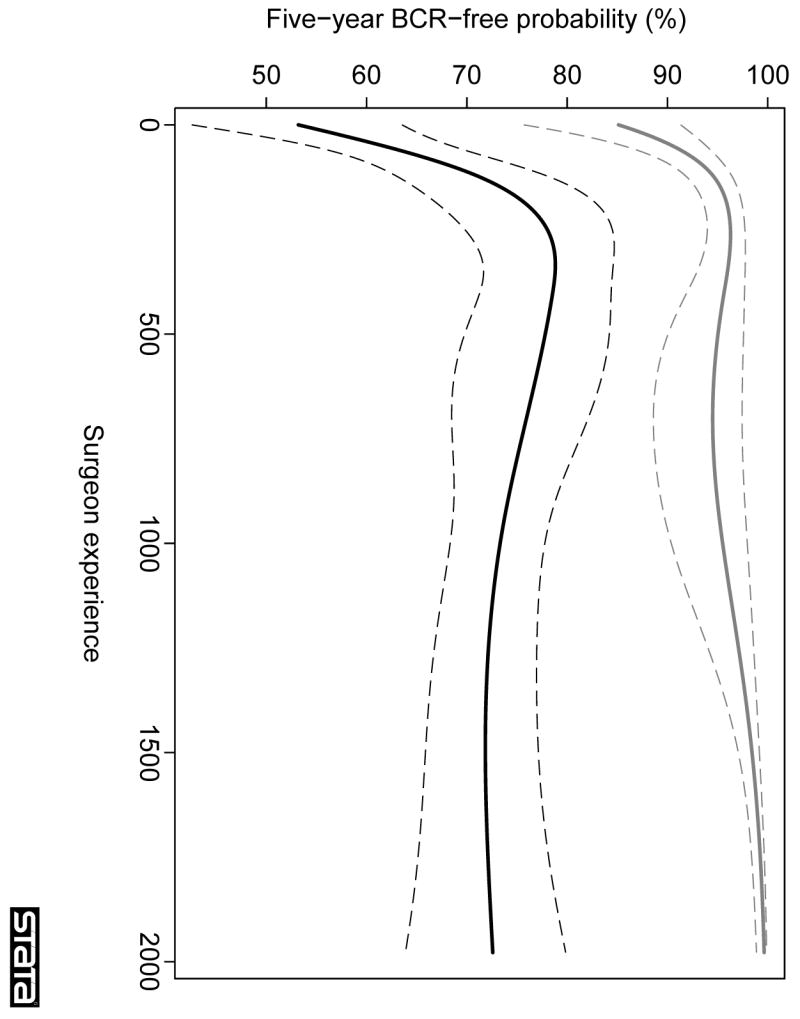
Methods: The study included 7765 eligible prostate cancer patients treated with open radical prostatectomy by one of 72 surgeons. Surgeon experience was coded as the total number of radical prostatectomies conducted by the surgeon prior to a patient's surgery. Multivariable regression models of survival time were used to evaluate the association between surgeon experience and biochemical recurrence, with adjustment for PSA, stage, and grade. Analyses were conducted separately for patients with organ-confined and locally advanced disease.
Results: Five-year recurrence-free probability for patients with organ-confined disease approached 100% for the most experienced surgeons. Conversely, the learning curve for patients with locally advanced disease reached a plateau at approximately 70%, suggesting that about a third of these patients cannot be cured by surgery alone.
Conclusions: Excellent rates of cancer control for patients with organ-confined disease treated by the most experienced surgeons suggest that the primary reason such patients recur is inadequate surgical technique.
Figures
Comment in
-
Cancer-related outcome and learning curve in retropubic radical prostatectomy: "if you need an operation, the most important step is to choose the right surgeon".Eur Urol. 2008 May;53(5):874-6. doi: 10.1016/j.eururo.2008.01.087. Epub 2008 Feb 8. Eur Urol. 2008. PMID: 18276062 No abstract available.
-
Words of wisdom. Re: effects of pathologic stage on the learning curve for radical prostatectomy: evidence that recurrence in organ-confined cancer is largely related to inadequate surgical technique.Eur Urol. 2008 Nov;54(5):1203-4. doi: 10.1016/j.eururo.2008.07.068. Eur Urol. 2008. PMID: 19051384 No abstract available.
References
-
- Halm EA, Lee C, Chassin MR. Is volume related to outcome in health care? A systematic review and methodologic critique of the literature. Ann Intern Med. 2002;137:511–20. - PubMed
-
- Begg CB, Riedel ER, Bach PB, et al. Variations in morbidity after radical prostatectomy. N Engl J Med. 2002;346:1138–44. - PubMed
-
- Hu JC, Gold KF, Pashos CL, Mehta SS, Litwin MS. Role of surgeon volume in radical prostatectomy outcomes. J Clin Oncol. 2003;21:401–5. - PubMed
-
- Van Poppel H, Boulanger SF, Joniau S. Quality assurance issues in radical prostatectomy. Eur J Surg Oncol. 2005;31:650–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
