

Patterns of locoregional recurrence after surgery and radiotherapy or chemoradiation for rectal cancer
- PMID: 18207667
- PMCID: PMC6455925
- DOI: 10.1016/j.ijrobp.2007.11.018
Patterns of locoregional recurrence after surgery and radiotherapy or chemoradiation for rectal cancer
Abstract
Purpose: To identify patterns of locoregional recurrence in patients treated with surgery and preoperative or postoperative radiotherapy or chemoradiation for rectal cancer.
Methods and materials: Between November 1989 and October 2001, 554 patients with rectal cancer were treated with surgery and preoperative (85%) or postoperative (15%) radiotherapy, with 95% receiving concurrent chemotherapy. Among these patients, 46 had locoregional recurrence as the first site of failure. Computed tomography images showing the site of recurrence and radiotherapy simulation films were available for 36 of the 46 patients. Computed tomography images were used to identify the sites of recurrence and correlate the sites to radiotherapy fields in these 36 patients.
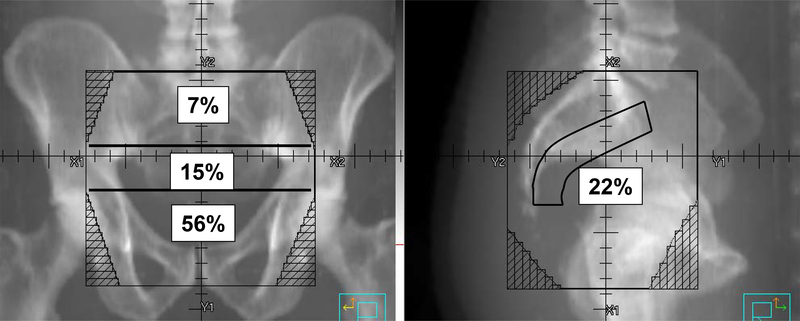
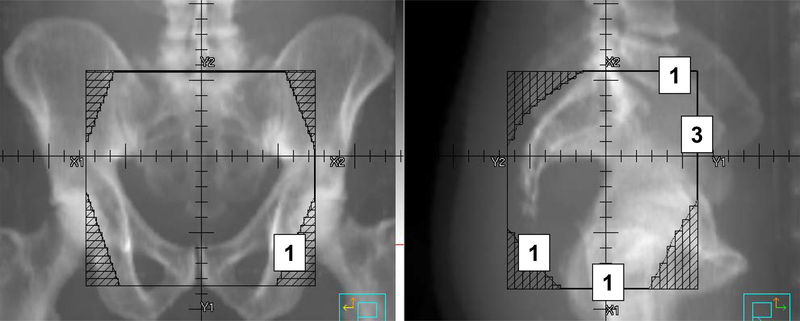
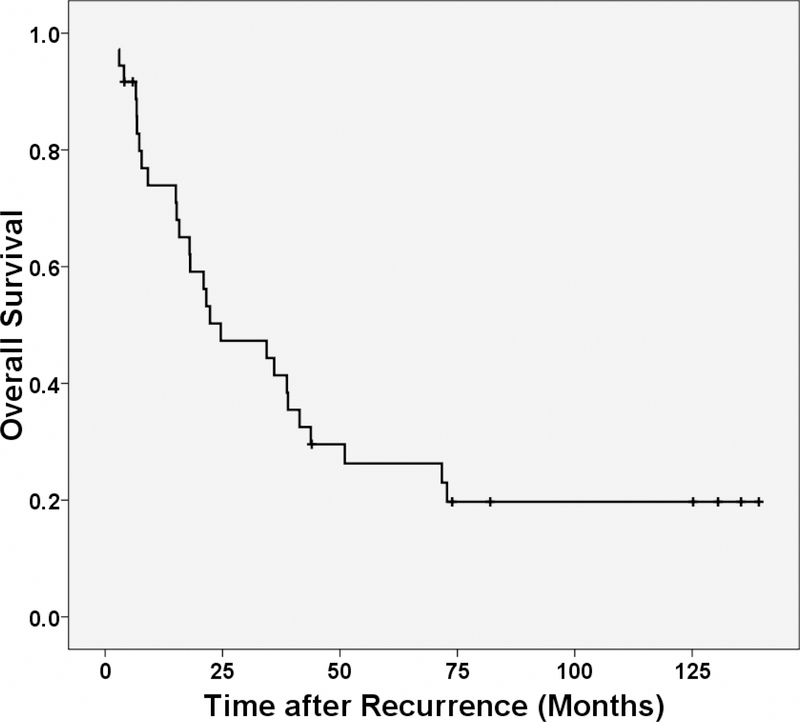
Results: The estimated 5-year locoregional control rate was 91%. The 36 patients in the study had locoregional recurrences at 43 sites. There were 28 (65%) in-field, 7 (16%) marginal, and 8 (19%) out-of-field recurrences. Among the in-field recurrences, 15 (56%) occurred in the low pelvis, 6 (22%) in the presacral region, 4 (15%) in the mid-pelvis, and 2 (7%) in the high pelvis. Clinical T stage, pathologic T stage, and pathologic N stage were significantly associated with the risk of in-field locoregional recurrence. The median survival after locoregional recurrence was 24.6 months.
Conclusions: Patients treated with surgery and radiotherapy or chemoradiation for rectal cancer had a low risk of locoregional recurrence, with the majority of recurrences occurring within the radiation field. Because 78% of in-field recurrences occur in the low pelvic and presacral regions, consideration should be given to including the low pelvic and presacral regions in the radiotherapy boost field, especially in patients at high risk of recurrence.
Conflict of interest statement
CONFLICT OF INTEREST NOTIFICATION:
Actual and potential conflicts of interest do not exist.
Figures
Comment in
-
Radiation fields of neoadjuvant concurrent chemoradiotherapy for rectal cancer: in regard to Yu et al. (Int J Radiat Oncol Biol Phys 2008;71:1175-1180).Int J Radiat Oncol Biol Phys. 2009 Feb 1;73(2):639; author reply 639-40. doi: 10.1016/j.ijrobp.2008.09.033. Int J Radiat Oncol Biol Phys. 2009. PMID: 19147033 No abstract available.
References
-
- Anonymous. Prolongation of the disease-free interval in surgically treated rectal carcinoma. Gastrointestinal Tumor Study Group. N Engl J Med 1985;312:1465–1472. - PubMed
-
- Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 1991;324:709–715. - PubMed
-
- O’ Connell M, Martenson JA, Wieand HS, et al. Improving adjuvant therapy for rectal cancer by combining protracted-infusion fluorouracil with radiation therapy after curative surgery. N Engl J Med 1994;331:502–507. - PubMed
-
- Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351:1731–1740. - PubMed
-
- Wolmark N, Wieand HS, Hyams DM, et al. Randomized trial of postoperative adjuvant chemotherapy with or without radiotherapy for carcinoma of the rectum: National Surgical Adjuvant Breast and Bowel Project Protocol R-02. J Natl Cancer Inst 2000;92:388–396. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
