

Just what the doctor ordered. Review of the evidence of the impact of computerized physician order entry system on medication errors
- PMID: 18211517
- PMCID: PMC2323150
- DOI: 10.1111/j.1475-6773.2007.00751.x
Just what the doctor ordered. Review of the evidence of the impact of computerized physician order entry system on medication errors
Abstract
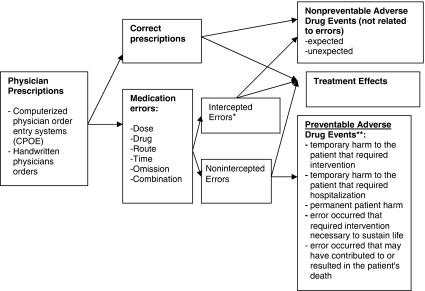
Objective: To examine the association between computerization of physician orders and prescribing medication errors. Data Sources. Studies published in English language were identified through MEDLINE (1990 through December 2005), Cochrane Central Register of Controlled Trials, and bibliographies of retrieved articles. Of 252 identified in the search, 12 (4.8 percent) original investigations that compared rates of prescribing medication errors with handwritten and computerized physician orders were included.
Data collection: Information on study design, participant characteristics, clinical settings, and outcomes rates were abstracted independently by two investigators using a standardized protocol.
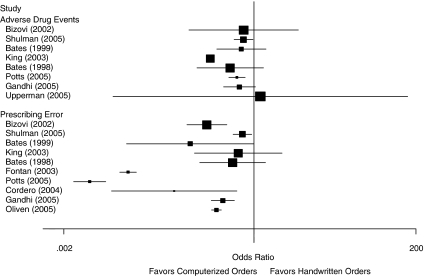
Principal findings: Compared with handwritten orders, 80 percent of studies (8/10 studies) reported a significant reduction in total prescribing errors, 43 percent in dosing errors (3/7 studies), and 37.5 percent in adverse drug events (3/8 studies). The use of computerized orders was associated with a 66 percent reduction in total prescribing errors in adults (odds ratio [OR]=0.34; 95 percent confidence interval [CI] 0.22-0.52) and a positive tendency in children (p for interaction=.028). The benefit of computerized orders was larger when the rate of errors was more than 12 percent with handwritten orders (p for interaction=.022). Significant heterogeneity in the results compromised pooled relative risks. One randomized controlled intervention demonstrated the greatest benefits of computerized orders on total prescribing errors (OR=0.02, 95 percent CI 0.01-0.02) and dosing errors (OR=0.28; 95 percent CI 0.15-0.52) with 775 avoided prescribing errors (95 percent CI 752-811) per 1,000 orders in a pediatric hospital.
Conclusions: Computerization of physicians' orders shows great promise. It will be more effective when linked to other computerized systems to detect and prevent prescribing errors.
Figures
References
-
- Aspden P Institute of Medicine (U.S.) Committee on Identifying and Preventing Medication Errors. Preventing Medication Errors. Washington, DC: National Academies Press; 2007.
-
- Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, Laffel G, Sweitzer BJ, Shea BF, Hallisey R, Vander Vliet M, Nemeskal R, Leape LL. Incidence of Adverse Drug Events and Potential Adverse Drug Events. Implications for Prevention. ADE Prevention Study Group. Journal of the American Medical Association. 1995b;274(1):29–34. - PubMed
-
- Bates DW, Leape LL, Cullen DJ, Laird N, Petersen LA, Teich JM, Burdick E, Hickey M, Kleefield S, Shea B, Vander Vliet M, Seger DL. Effect of Computerized Physician Order Entry and a Team Intervention on Prevention of Serious Medication Errors. Journal of the American Medical Association. 1998;280(15):1311–6. - PubMed
-
- Bates DW, Spell N, Cullen DJ, Burdick E, Laird N, Petersen LA, Small SD, Sweitzer BJ, Leape LL. The Costs of Adverse Drug Events in Hospitalized Patients. Adverse Drug Events Prevention Study Group. Journal of the American Medical Association. 1997;277(4):307–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
