

Clinical response and outcome of infection with Salmonella enterica serotype Typhi with decreased susceptibility to fluoroquinolones: a United States foodnet multicenter retrospective cohort study
- PMID: 18212096
- PMCID: PMC2292528
- DOI: 10.1128/AAC.01509-07
Clinical response and outcome of infection with Salmonella enterica serotype Typhi with decreased susceptibility to fluoroquinolones: a United States foodnet multicenter retrospective cohort study
Abstract
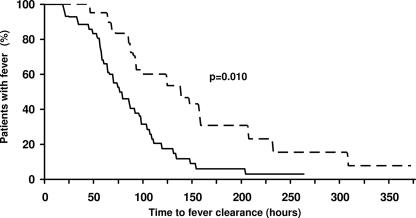
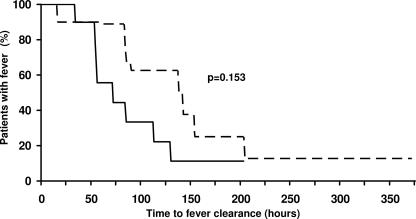
Patients with typhoid fever due to Salmonella enterica serotype Typhi strains for which fluoroquinolones MICs are elevated yet that are classified as susceptible by the current interpretive criteria of the Clinical and Laboratory Standards Institute may not respond adequately to fluoroquinolone therapy. Patients from seven U.S. states with invasive Salmonella serotype Typhi infection between 1999 and 2002 were enrolled in a multicenter retrospective cohort study. Patients infected with Salmonella serotype Typhi isolates with ciprofloxacin MICs of 0.12 to 1 microg/ml (decreased ciprofloxacin susceptibility but not resistant to ciprofloxacin [DCS]) were compared with patients infected with isolates with ciprofloxacin MICs <0.12 microg/ml for fever clearance time and treatment failure. Of 71 patients, 30 (43%) were female and 24 (34%) were infected with Salmonella serotype Typhi with DCS; the median age was 14 years (range, 1 to 51 years). Twenty-one (88%) of 24 isolates with DCS were resistant to nalidixic acid. The median antimicrobial-related fever clearance times in the DCS and non-DCS groups were 92 h (range, 21 to 373 h) and 72 h (range, 19 to 264 h) (P = 0.010), respectively, and the fluoroquinolone-related fever clearance times in the DCS and non-DCS groups were 90 h (range, 9 to 373 h) and 64 h (range, 34 to 204 h) (P = 0.153), respectively. Four (17%) of 24 patients in the DCS group and 2 (4%) of 46 patients in the non-DCS group (relative risk, 2.5; 95% confidence interval, 1.2 to 5.1) experienced treatment failure. Associations persisted after adjustment for potential confounders. We demonstrate that patients infected with Salmonella serotype Typhi isolates with DCS show evidence of a longer time to fever clearance and more frequent treatment failure. Nalidixic acid screening does not detect all isolates with DCS.
Figures
References
-
- Ackers, M.-L., N. D. Puhr, R. V. Tauxe, and E. D. Mintz. 2000. Laboratory-based surveillance of Salmonella serotype Typhi infections in the United States: antimicrobial resistance on the rise. JAMA 283:2668-2673. - PubMed
-
- Allos, B. M., M. R. Moore, P. M. Griffin, and R. V. Tauxe. 2004. Surveillance for sporadic foodborne disease in the 21st century: the FoodNet perspective. Clin. Infect. Dis. 38(Suppl. 3):S115-S120. - PubMed
-
- Biedenbach, D. J., M. Toleman, T. R. Walsh, and R. N. Jones. 2006. Analysis of Salmonella spp. with resistance to extended-spectrum cephalosporins and fluoroquinolones isolated in North America and Latin America: report from the SENTRY antimicrobial surveillance program (1997-2004). Diagn. Microbiol. Infect. Dis. 54:13-21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
