

En bloc spondylectomy in malignant tumors of the spine
- PMID: 18214553
- PMCID: PMC2295282
- DOI: 10.1007/s00586-008-0599-8
En bloc spondylectomy in malignant tumors of the spine
Abstract
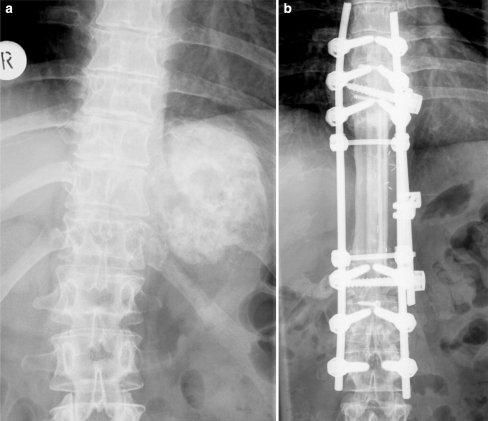
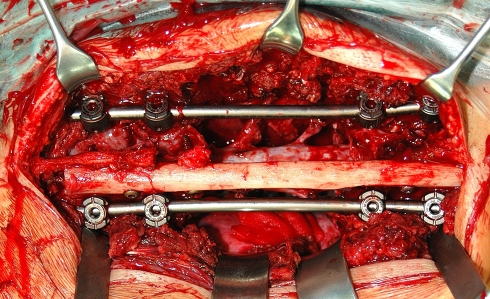
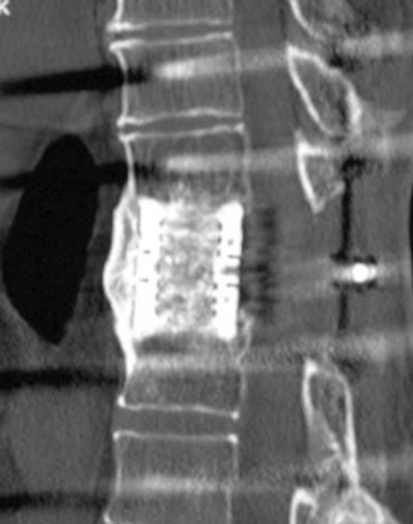
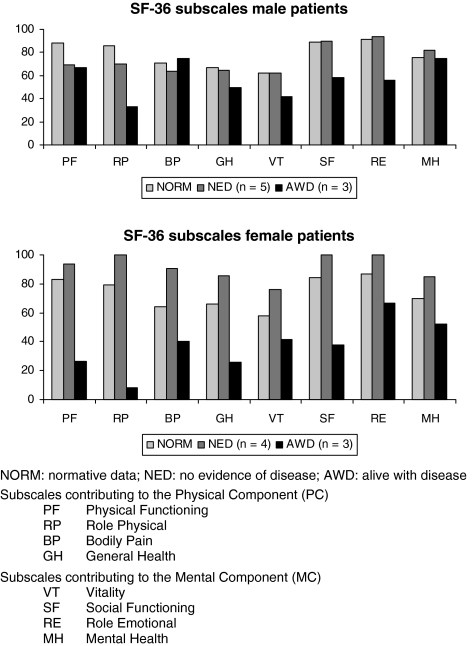
En bloc spondylectomy is a technique that enables wide or marginal resection of malignant lesions of the spine. Both all posterior techniques as well as combined approaches are reported. Aim of the present study was to analyse the results of 21 patients with malignant lesions of the spine, all treated with en bloc excision in a combined posteroanterior (n = 19) or all posterior approach (n = 2). Twenty-one consecutive patients, operated between 1997 and 2005, were included into this retrospective study. Thirteen patients had primary malignant lesions, eight patients had solitary metastases, all located in the thoracolumbar spine. There were 16 single level, three two-level, one three-level and one four-level spondylectomy. The patients were followed clinically and radiographically (including CT studies) with an average follow-up of 4 years. Out of 11 patients with primary Ewing or osteosarcoma seven patients are alive without any evidence of disease. One patient died after 5 years from other causes and three are alive with evidence of disease. Latter had either a poor histologic response to the preoperative chemotherapy (n = 2) or an intralesional resection (n = 1). All three patients with solitary spinal metastases of Ewing or osteosarcoma died of the disease. Five patients with solitary metastases of mainly hypernephroma are alive. In total, six resections were intralesional, mainly due to large intraspinal tumor masses, with two patients having had previous surgery. In the remaining cases, wide (n = 10) or marginal (n = 5) resection was accomplished. There were one pseudarthrosis requiring extension of the fusion and two cases with local recurrences and repeated excisional surgery. At follow-up CT studies, all cages were fused. Health related quality of life analysis (SF-36) revealed only slightly decreased physical component and normal mental component scores compared to normals in those patients with no evidence of disease. En bloc spondylectomy enables wide or marginal resection of malignant lesions of the spine in most cases with acceptable morbidity. Intralesional resection, poor histologic response, and solitary spinal metastases of Ewing and osteosarcoma are associated with a poor prognosis.
Figures
References
-
- Bielack SS, Kempf-Bielack B, Delling G, Exner G, Flege S, et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol. 2002;1:776–790. doi: 10.1200/JCO.20.3.776. - DOI - PubMed
-
- Ellert U, Bellach B. German national health survey 1998—description of an update random sampling test. Gesundheitswesen. 1999;61:S184–S190. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
