

Costs of allogeneic hematopoietic cell transplantation with high-dose regimens
- PMID: 18215780
- PMCID: PMC2259445
- DOI: 10.1016/j.bbmt.2007.10.010
Costs of allogeneic hematopoietic cell transplantation with high-dose regimens
Abstract
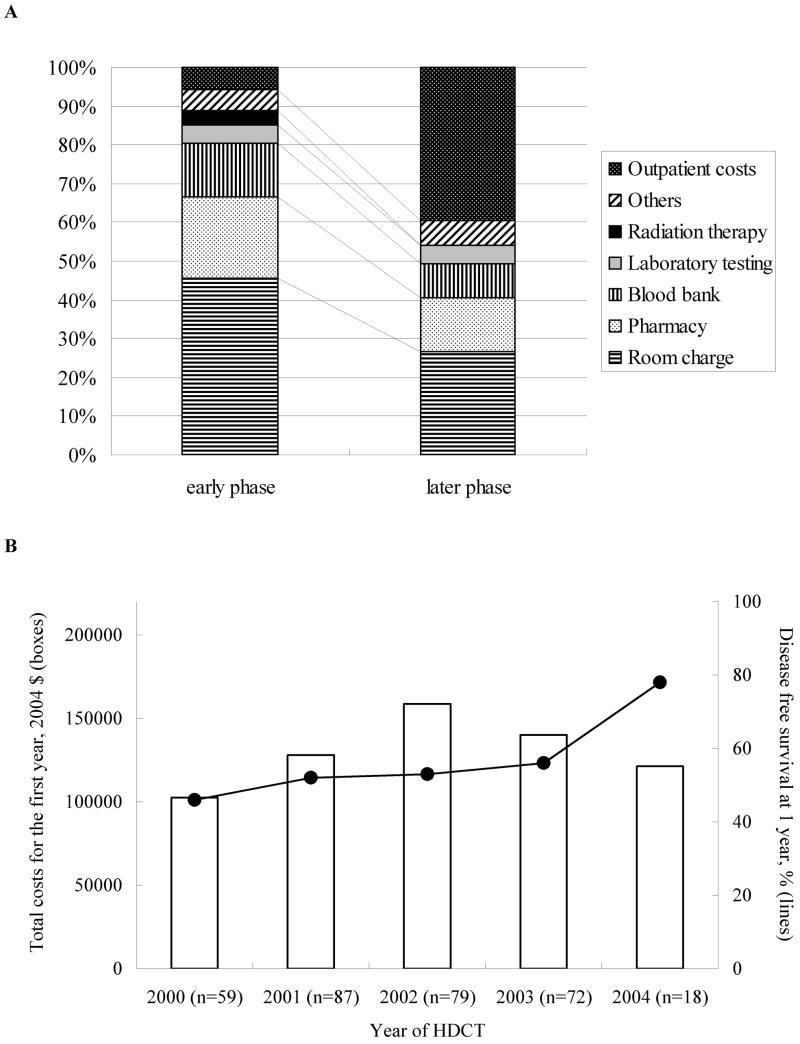
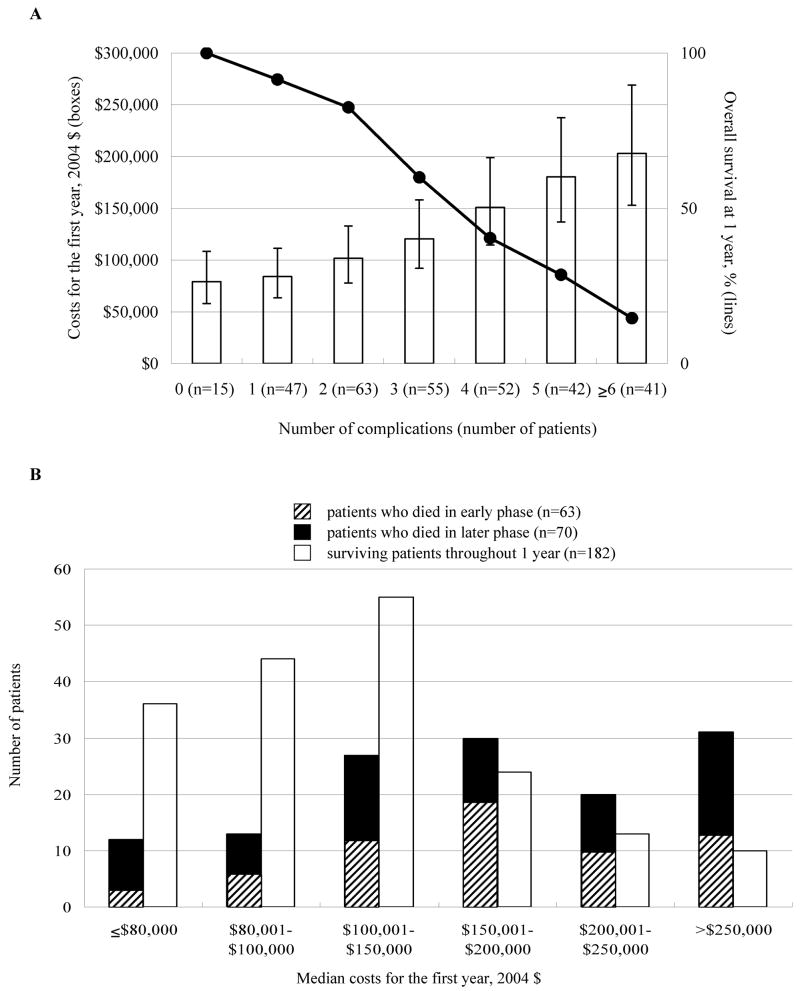
To characterize the costs of allogeneic hematopoietic cell transplantation with high-dose regimens (HDCT), we analyzed clinical information and costs of 315 HDCT recipients during a 4-year study period beginning in 2000. Multivariate analyses were performed to identify pre- and/or post-HDCT factors predicting higher costs within the first year. Overall survival (OS) at 100 days and 1 year were 80% and 58%, respectively. The median cost and days of hospitalization were $102,574 in 2004 US dollars and 36 days in the hospital for 100 days, and $128,800 and 39 days in the hospital for 1 year. Early costs, defined as costs within the first 100 days, accounted for 84% of total costs within the first year. Inpatient costs comprise 94% of the early costs, but only 61% of the later costs defined as costs incurred between 101 days and 1 year. Of the pre-HDCT factors, unrelated donors and advanced disease risk were significantly associated with increased cost. When post-HDCT events were also considered, these pre-HDCT factors were no longer independently predictive of high cost. Instead, severe complications post-HDCT were associated with higher costs, increasing total costs $20,228 on average. If no complications occurred, the mean cost within the first year was $79,222. These results provide cost estimates for complicated and uncomplicated HDCT procedures, as well as costs for management of specific transplant complications.
Figures
References
-
- Thomas ED, Lochte HL, Jr, Lu WC, Ferrebee JW. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. N Engl J Med. 1957;257:491–496. - PubMed
-
- Mielcarek M, Martin PJ, Leisenring W, et al. Graft-versus-host disease after nonmyeloablative versus conventional hematopoietic stem cell transplantation. Blood. 2003;102:756–762. - PubMed
-
- Sparrelid E, Hagglund H, Remberger M, et al. Risk factors for septicemia during aplastic period after allogeneic bone marrow transplantation. Transplant Proc. 1995;27:3530. - PubMed
-
- Hebart H, Loffler J, Meisner C, et al. Early detection of aspergillus infection after allogeneic stem cell transplantation by polymerase chain reaction screening. J Infect Dis. 2000;181:1713–1719. - PubMed
-
- Ljungman P, Lore K, Aschan J, et al. Use of a semi-quantitative PCR for cytomegalovirus DNA as a basis for pre-emptive antiviral therapy in allogeneic bone marrow transplant patients. Bone Marrow Transplant. 1996;17:583–587. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
