

Parallel processing of nociceptive A-delta inputs in SII and midcingulate cortex in humans
- PMID: 18216202
- PMCID: PMC6670999
- DOI: 10.1523/JNEUROSCI.2934-07.2008
Parallel processing of nociceptive A-delta inputs in SII and midcingulate cortex in humans
Abstract
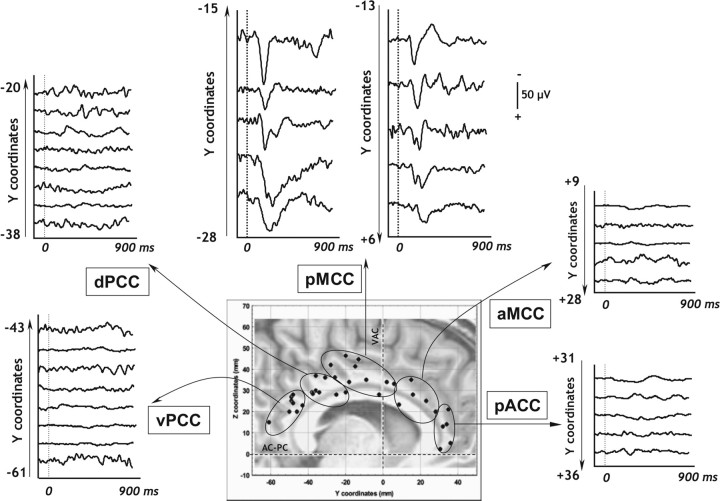
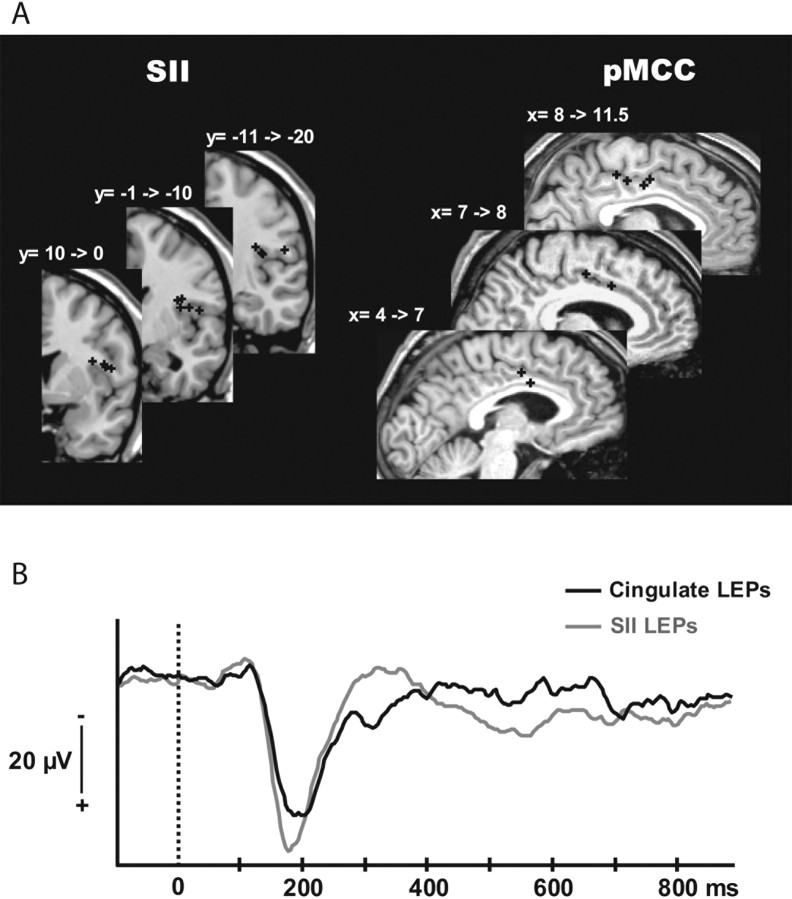
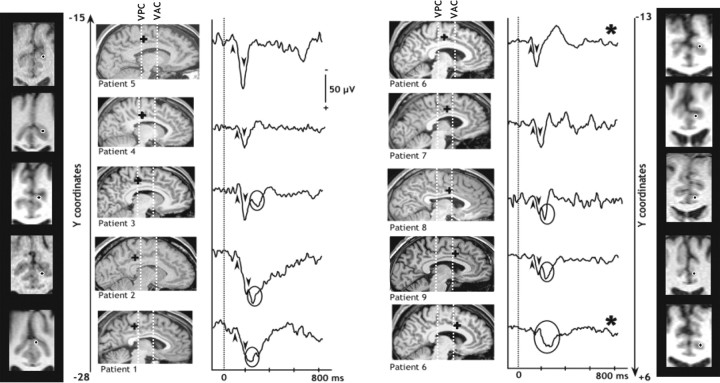
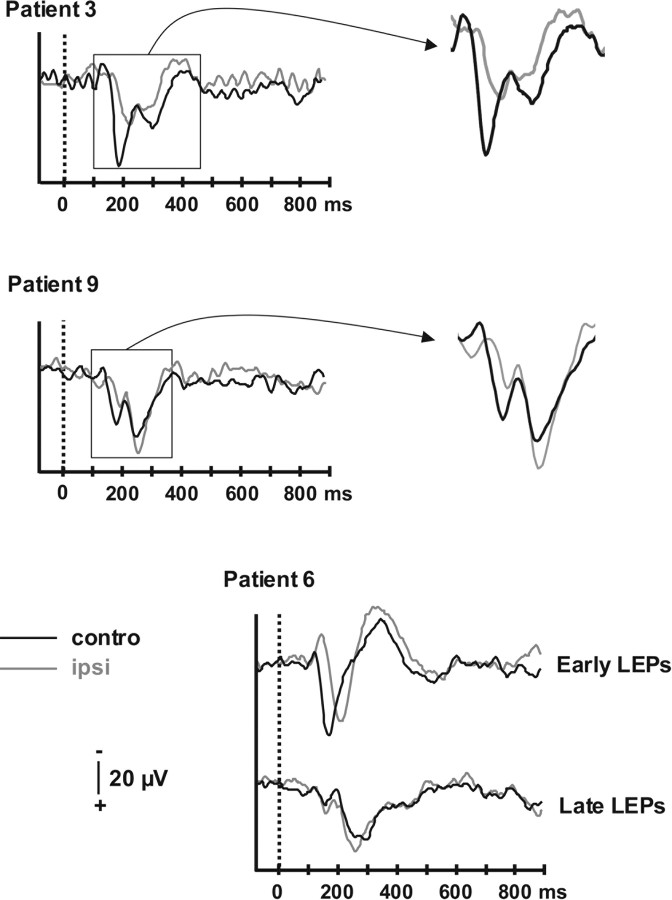
The cingulate cortex (CC) as a part of the "medial" pain subsystem is generally assumed to be involved in the affective and/or cognitive dimensions of pain processing, which are viewed as relatively slow processes compared with the sensory-discriminative pain coding by the lateral second somatosensory area (SII)-insular cortex. The present study aimed at characterizing the location and timing of the CC evoked responses during the 1 s period after a painful laser stimulus, by exploring the whole rostrocaudal extent of this cortical area using intracortical recordings in humans. Only a restricted area in the median CC region responded to painful stimulation, namely the posterior midcingulate cortex (pMCC), the location of which is consistent with the so-called "motor CC" in monkeys. Cingulate pain responses showed two components, of which the earliest peaked at latencies similar to those obtained in SII. These data provide direct evidence that activations underlying the processing of nociceptive information can occur simultaneously in the "medial" and "lateral" subsystems. The existence of short-latency pMCC responses to pain further indicates that the "medial pain system" is not devoted exclusively to the processing of emotional information, but is also involved in fast attentional orienting and motor withdrawal responses to pain inputs. These functions are, not surprisingly, conducted in parallel with pain intensity coding and stimulus localization specifically subserved by the sensory-discriminative "lateral" pain system.
Figures
References
-
- Adriaensen H, Gybels J, Handwerker HO, Van Hees J. Response properties of thin myelinated (A-delta) fibers in human skin nerves. J Neurophysiol. 1983;49:111–122. - PubMed
-
- Albe-Fessard D, Berkley KJ, Kruger L, Ralston HJ, III, Willis WD., Jr Diencephalic mechanisms of pain sensation. Brain Res. 1985;356:217–296. - PubMed
-
- Apkarian VA, Hodge CJ. Primate spinothalamic pathways: I. A quantitative study of the cells of origin of the spinothalamic pathway. J Comp Neurol. 1989;288:447–473. - PubMed
-
- Baleydier C, Mauguière F. The duality of the cingulate gyrus in monkey—neuroanatomical study and functional hypothesis. Brain. 1980;103:525–554. - PubMed
-
- Bastuji H, Perchet C, Legrain V, Montes C, Garcia-Larrea L. Laser evoked responses to painful stimulation persist during sleep and predict subsequent arousals. Pain. 2008 in press. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical