

A comparison of bare-metal and drug-eluting stents for off-label indications
- PMID: 18216354
- PMCID: PMC2761092
- DOI: 10.1056/NEJMoa0706258
A comparison of bare-metal and drug-eluting stents for off-label indications
Abstract
Background: Recent reports suggest that off-label use of drug-eluting stents is associated with an increased incidence of adverse events. Whether the use of bare-metal stents would yield different results is unknown.
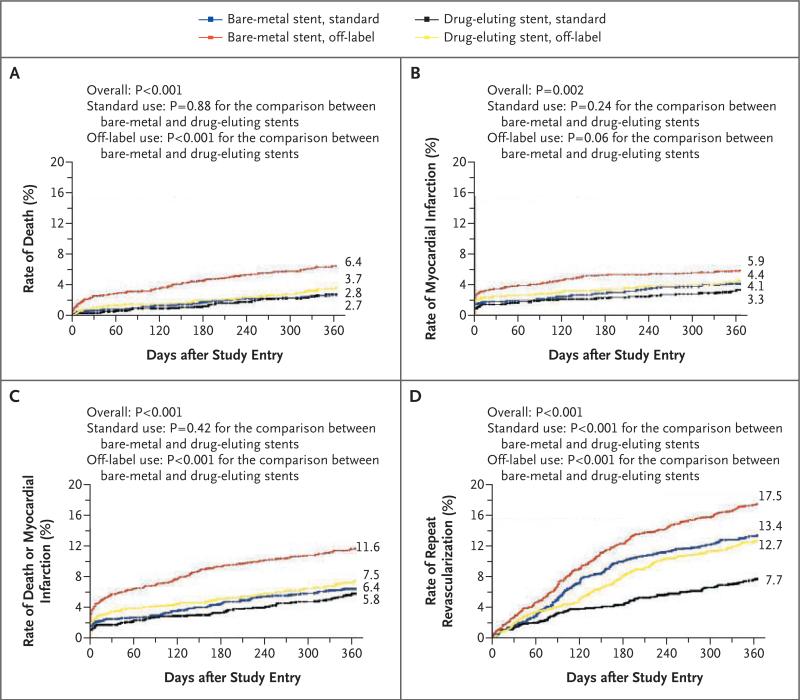
Methods: We analyzed data from 6551 patients in the National Heart, Lung, and Blood Institute Dynamic Registry according to whether they were treated with drug-eluting stents or bare-metal stents and whether use was standard or off-label. Patients were followed for 1 year for the occurrence of cardiovascular events and death. Off-label use was defined as use in restenotic lesions, lesions in a bypass graft, left main coronary artery disease, or ostial, bifurcated, or totally occluded lesions, as well as use in patients with a reference-vessel diameter of less than 2.5 mm or greater than 3.75 mm or a lesion length of more than 30 mm.
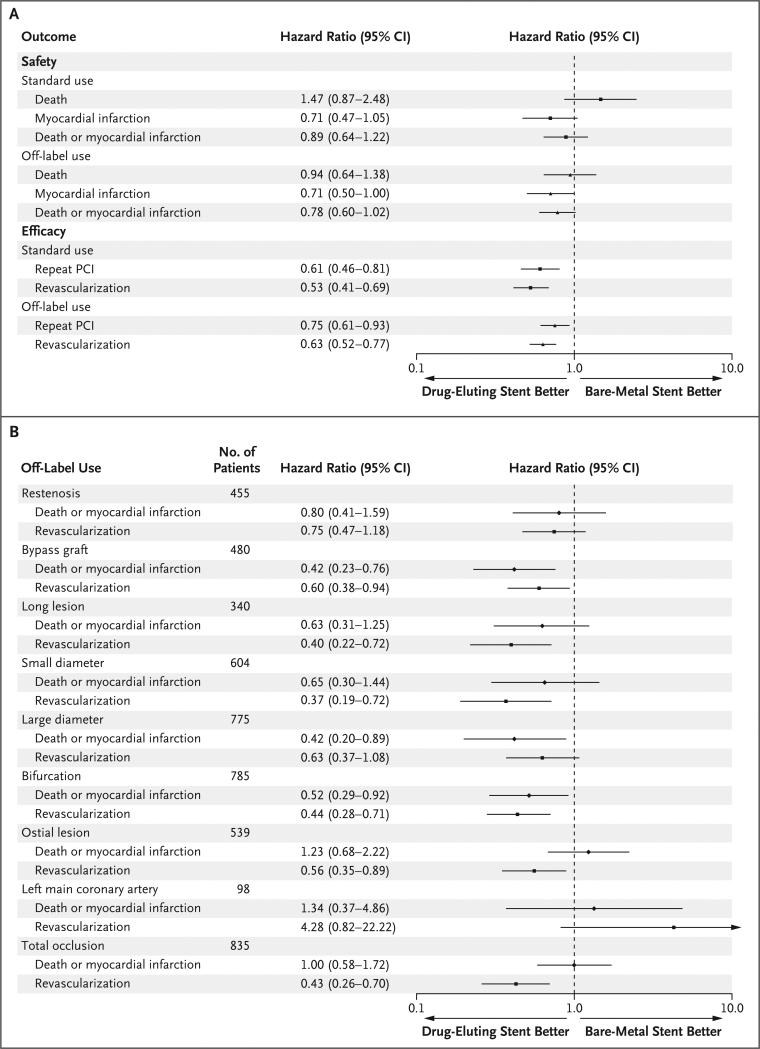
Results: Off-label use occurred in 54.7% of all patients with bare-metal stents and 48.7% of patients with drug-eluting stents. As compared with patients with bare-metal stents, patients with drug-eluting stents had a higher prevalence of diabetes, hypertension, renal disease, previous percutaneous coronary intervention and coronary-artery bypass grafting, and multivessel coronary artery disease. One year after intervention, however, there were no significant differences in the adjusted risk of death or myocardial infarction in patients with drug-eluting stents as compared with those with bare-metal stents, whereas the risk of repeat revascularization was significantly lower among patients with drug-eluting stents.
Conclusions: Among patients with off-label indications, the use of drug-eluting stents was not associated with an increased risk of death or myocardial infarction but was associated with a lower rate of repeat revascularization at 1 year, as compared with bare-metal stents. These findings support the use of drug-eluting stents for off-label indications.
Copyright 2008 Massachusetts Medical Society.
Figures
Comment in
-
Bare-metal versus drug-eluting coronary stents.N Engl J Med. 2008 Jun 5;358(23):2516; author reply 2517-8. doi: 10.1056/NEJMc080369. N Engl J Med. 2008. PMID: 18525053 No abstract available.
-
Bare-metal versus drug-eluting coronary stents.N Engl J Med. 2008 Jun 5;358(23):2516-7; author reply 2517-8. N Engl J Med. 2008. PMID: 18536096 No abstract available.
References
-
- Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346:1773–80. - PubMed
-
- Colombo A, Drzewiecki J, Banning A, et al. Randomized study to assess the effectiveness of slow- and moderate-release polymer-based paclitaxel-eluting stents for coronary artery lesions. Circulation. 2003;108:788–94. - PubMed
-
- Grube E, Silber S, Hauptmann KE, et al. TAXUS I: six- and twelve-month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation. 2003;107:38–42. - PubMed
-
- Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349:1315–23. - PubMed
-
- Schofer J, Schlüter M, Gershlick AH, et al. Sirolimus-eluting stents for treatment of patients with long atherosclerotic lesions in small coronary arteries: double-blind, randomized controlled trial (E-SIRIUS). Lancet. 2003;362:1093–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials