

Debridement and closed packing for sterile or infected necrotizing pancreatitis: insights into indications and outcomes in 167 patients
- PMID: 18216536
- PMCID: PMC3806106
- DOI: 10.1097/SLA.0b013e31815b6976
Debridement and closed packing for sterile or infected necrotizing pancreatitis: insights into indications and outcomes in 167 patients
Abstract
Objective: To examine the surgical indications and clinical outcomes of a large cohort of patients with necrotizing pancreatitis.
Summary background data: Mortality after debridement for necrotizing pancreatitis continues to be inordinately high. The clinical experience with patients who underwent uniform surgical treatment for necrotizing pancreatitis at the Massachusetts General Hospital over a 15-year period is described.
Methods: Retrospective review of 167 patients with necrotizing pancreatitis who required intervention and were treated with single stage debridement and a closed packing technique. Particular emphasis was placed on the indication for surgery and the presence of infected necrosis. Multiple logistic regression models were used to identify predictors of mortality.
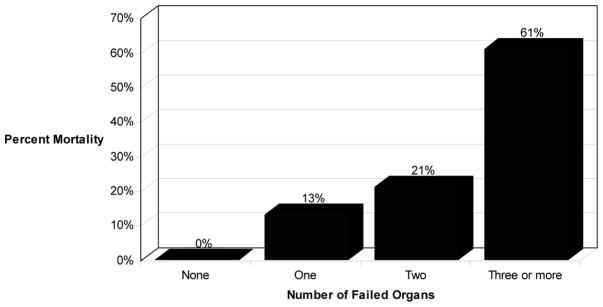
Results: The primary preoperative indication for operation was infected necrosis (51%), but intraoperative cultures proved that 72% of the entire cohort was infected. The rate of reoperation was 12.6%, and 29.9% of patients required percutaneous interventional radiology drainage after initial debridement. Overall operative mortality was 11.4% (19/167), but higher in patients who were operated upon before 28 days (20.3% vs. 5.1%, P = 0.002). Other important predictors of mortality included organ failure > or =3 (OR = 2.4, P = 0.001), postoperative intensive care unit stay > or =6 days (OR = 15.9, P = 0.001), and female gender (OR = 5.41, P = 0.02).
Conclusions: Open, transperitoneal debridement followed by closed packing and drainage results in the lowest reported mortality and reoperation rates, and provides a standard for comparing other methods of treatment. A negative FNA does not reliably rule out infection. The clinical status of the patients and not proof of infection should determine the need for debridement.
Figures
References
-
- Beger HG, Rau B, Isenmann R. Natural history of necrotizing pancreatitis. Pancreatology. 2003;3:93–101. - PubMed
-
- Bradley EL, III, Allen K. A prospective longitudinal study of observation versus surgical intervention in the management of necrotizing pancreatitis. Am J Surg. 1991;161:19–24. discussion-5. - PubMed
-
- Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142–2150. - PubMed
-
- Connor S, Alexakis N, Raraty MG, et al. Early and late complications after pancreatic necrosectomy. Surgery. 2005;137:499–505. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
