

The effect of offering different numbers of colorectal cancer screening test options in a decision aid: a pilot randomized trial
- PMID: 18218084
- PMCID: PMC2259331
- DOI: 10.1186/1472-6947-8-4
The effect of offering different numbers of colorectal cancer screening test options in a decision aid: a pilot randomized trial
Abstract
Background: Decision aids can improve decision making processes, but the amount and type of information that they should attempt to communicate is controversial. We sought to compare, in a pilot randomized trial, two colorectal cancer (CRC) screening decision aids that differed in the number of screening options presented.
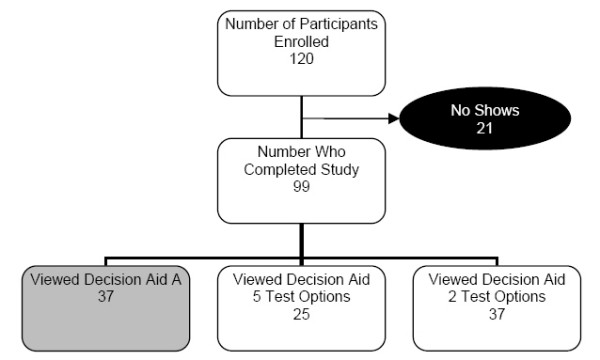
Methods: Adults ages 48-75 not currently up to date with screening were recruited from the community and randomized to view one of two versions of our previously tested CRC screening decision aid. The first version included five screening options: fecal occult blood test (FOBT), sigmoidoscopy, a combination of FOBT and sigmoidoscopy, colonoscopy, and barium enema. The second discussed only the two most frequently selected screening options, FOBT and colonoscopy. Main outcomes were differences in screening interest and test preferences between groups after decision aid viewing. Patient test preference was elicited first without any associated out-of-pocket costs (OPC), and then with the following costs: FOBT-$10, sigmoidoscopy-$50, barium enema-$50, and colonoscopy-$200.
Results: 62 adults participated: 25 viewed the 5-option decision aid, and 37 viewed the 2-option version. Mean age was 54 (range 48-72), 58% were women, 71% were White, 24% African-American; 58% had completed at least a 4-year college degree. Comparing participants that viewed the 5-option version with participants who viewed the 2-option version, there were no differences in screening interest after viewing (1.8 vs. 1.9, t-test p = 0.76). Those viewing the 2-option version were somewhat more likely to choose colonoscopy than those viewing the 5-option version when no out of pocket costs were assumed (68% vs. 46%, p = 0.11), but not when such costs were imposed (41% vs. 42%, p = 1.00).
Conclusion: The number of screening options available does not appear to have a large effect on interest in colorectal cancer screening. The effect of offering differing numbers of options may affect test choice when out-of-pocket costs are not considered.
References
-
- Increased use of colorectal cancer tests – United States, 2002 and 2004. Mmwr. 2006;55:308–311. - PubMed
-
- Screening for colorectal cancer: recommendation and rationale. Annals of internal medicine. 2002;137:129–131. - PubMed
-
- Kim J, Whitney A, Hayter S, Lewis C, Campbell M, Sutherland L, Fowler B, Googe S, McCoy R, Pignone M. Development and initial testing of a computer-based patient decision aid to promote colorectal cancer screening for primary care practice. BMC medical informatics and decision making. 2005;5:36. doi: 10.1186/1472-6947-5-36. - DOI - PMC - PubMed
-
- Pignone M, Harris R, Kinsinger L. Videotape-based decision aid for colon cancer screening. A randomized, controlled trial. Annals of internal medicine. 2000;133:761–769. - PubMed
-
- Schwartz B. The Paradox of Choice: why more is less. HarperCollins. 2004.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
