

Alpha-adrenergic inhibition increases collateral circuit conductance in rats following acute occlusion of the femoral artery
- PMID: 18218679
- PMCID: PMC2375691
- DOI: 10.1113/jphysiol.2007.149567
Alpha-adrenergic inhibition increases collateral circuit conductance in rats following acute occlusion of the femoral artery
Abstract
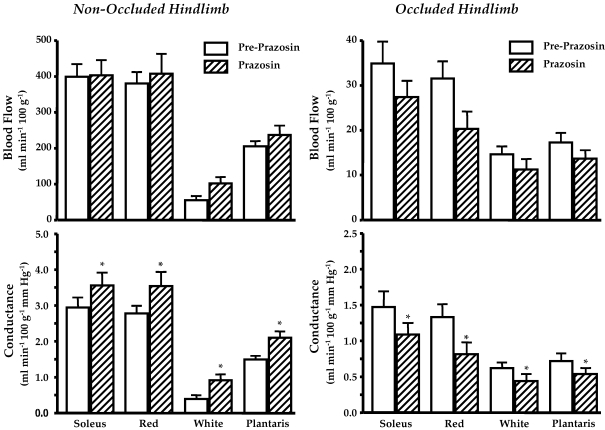
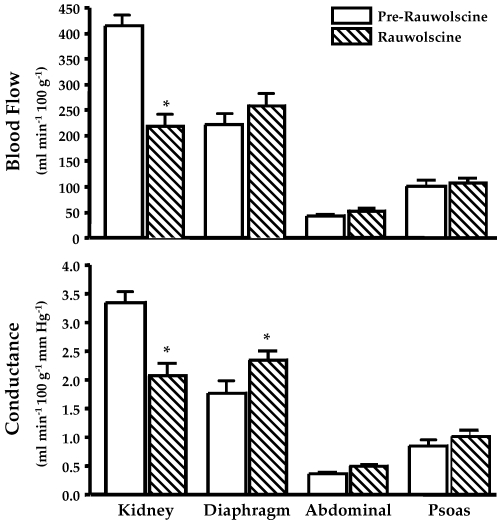
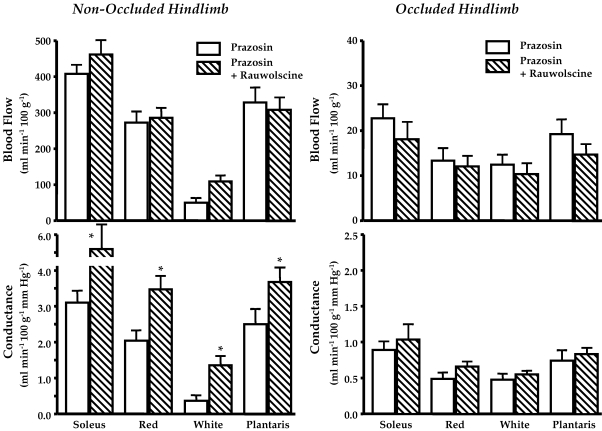
This study evaluated whether alpha-adrenergic activation contributes to collateral circuit vascular resistance in the hindlimb following acute unilateral occlusion of the femoral artery in rats. Blood pressures (BPs) were measured above (caudal artery) and below (distal femoral artery) the collateral circuit. Arterial BPs were reduced (15-35 mmHg) with individual (prazosin, rauwolscine) or combined (phentolamine) alpha-receptor inhibition. Blood flows (BFs) were measured using microspheres before and after alpha inhibition during the same treadmill speed. alpha(1) inhibition increased blood flow by approximately 40% to active muscles that were not affected by femoral occlusion, whereas collateral-dependent BFs to the calf muscles were reduced by 29 +/- 8.4% (P < 0.05), due to a decrease in muscle conductance with no change in collateral circuit conductance. alpha(2) inhibition decreased both collateral circuit (39 +/- 6.0%; P < 0.05) and calf muscle conductance (36 +/- 7.3%; P < 0.05), probably due to residual alpha(1) activation, since renal BF was markedly reduced with rauwolscine. Most importantly, inhibiting alpha(2) receptors in the presence of alpha(1) inhibition increased (43 +/- 12%; P < 0.05) collateral circuit conductance. Similarly, non-selective alpha inhibition with phentolamine increased collateral conductance (242 +/- 59%; P < 0.05). We interpret these findings to indicate that both alpha(1)- and alpha(2)-receptor activation can influence collateral circuit resistance in vivo during the high flow demands caused by exercise. Furthermore, we observed a reduced maximal conductances of active muscles that were ischaemic. Our findings imply that in the presence of excessive sympathetic activation, which can occur in the condition of intermittent claudication during exertion, an exaggerated vasoconstriction of the existing collateral circuit and active muscle will occur.
Figures











Similar articles
-
Training-induced vascular adaptations to ischemic muscle.J Physiol Pharmacol. 2008 Dec;59 Suppl 7(Suppl 7):57-70. J Physiol Pharmacol. 2008. PMID: 19258657 Free PMC article. Review.
-
Alpha-adrenergic and neuropeptide Y Y1 receptor control of collateral circuit conductance: influence of exercise training.J Physiol. 2008 Dec 15;586(24):5983-98. doi: 10.1113/jphysiol.2008.160101. Epub 2008 Nov 3. J Physiol. 2008. PMID: 18981031 Free PMC article.
-
Prior exercise training produces NO-dependent increases in collateral blood flow after acute arterial occlusion.Am J Physiol Heart Circ Physiol. 2002 Jan;282(1):H301-10. doi: 10.1152/ajpheart.00160.2001. Am J Physiol Heart Circ Physiol. 2002. PMID: 11748075
-
Sympathetic vasoconstriction in active skeletal muscles during dynamic exercise.J Appl Physiol (1985). 1997 Nov;83(5):1575-80. doi: 10.1152/jappl.1997.83.5.1575. J Appl Physiol (1985). 1997. PMID: 9375322
-
Neural control of muscle blood flow: importance during dynamic exercise.Clin Exp Pharmacol Physiol. 1997 Feb;24(2):117-25. doi: 10.1111/j.1440-1681.1997.tb01793.x. Clin Exp Pharmacol Physiol. 1997. PMID: 9075582 Review.
Cited by
-
Training-induced vascular adaptations to ischemic muscle.J Physiol Pharmacol. 2008 Dec;59 Suppl 7(Suppl 7):57-70. J Physiol Pharmacol. 2008. PMID: 19258657 Free PMC article. Review.
-
Low-frequency stimulation of group III and IV hind limb afferents evokes reflex pressor responses in decerebrate rats.Physiol Rep. 2016 Oct;4(20):e13001. doi: 10.14814/phy2.13001. Epub 2016 Oct 24. Physiol Rep. 2016. PMID: 27798354 Free PMC article.
-
Alpha-adrenergic and neuropeptide Y Y1 receptor control of collateral circuit conductance: influence of exercise training.J Physiol. 2008 Dec 15;586(24):5983-98. doi: 10.1113/jphysiol.2008.160101. Epub 2008 Nov 3. J Physiol. 2008. PMID: 18981031 Free PMC article.
-
Functional knockout of ASIC3 attenuates the exercise pressor reflex in decerebrated rats with ligated femoral arteries.Am J Physiol Heart Circ Physiol. 2020 May 1;318(5):H1316-H1324. doi: 10.1152/ajpheart.00137.2020. Epub 2020 Apr 17. Am J Physiol Heart Circ Physiol. 2020. PMID: 32302492 Free PMC article.
-
Femoral artery ligation increases the responses of thin-fiber muscle afferents to contraction.J Neurophysiol. 2015 Jun 1;113(10):3961-6. doi: 10.1152/jn.00288.2015. Epub 2015 Apr 8. J Neurophysiol. 2015. PMID: 25855694 Free PMC article.
References
-
- Bakke EF, Hisdal J, Jorgensen JJ, Kroese A, Stranden E. Blood pressure in patients with intermittent claudication increases continuously during walking. Eur J Vasc Endovasc Surg. 2007;33:2–25. - PubMed
-
- Buckwalter JB, Hamann JJ, Clifford PS. Neuropeptide Y1 receptor vasoconstriction in exercising canine skeletal muscles. J Appl Physiol. 2005;99:2115–2120. - PubMed
-
- Buckwalter JB, Mueller PJ, Clifford PS. Sympathetic vasoconstriction in active skeletal muscles during dynamic exercise. J Appl Physiol. 1997;83:1575–1580. - PubMed
-
- Buschmann I, Schaper W. Arteriogenesis versus angiogenesis: two mechanisms of vessel growth. News Physiol Sci. 1999;14:121–125. - PubMed
-
- Buschmann I, Schaper W. The pathophysiology of the collateral circulation (arteriogenesis) J Pathol. 2000;190:338–342. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous