

Effect of a 14-day course of systemic corticosteroids on the hypothalamic-pituitary-adrenal-axis in patients with acute exacerbation of chronic obstructive pulmonary disease
- PMID: 18221550
- PMCID: PMC2246097
- DOI: 10.1186/1471-2466-8-1
Effect of a 14-day course of systemic corticosteroids on the hypothalamic-pituitary-adrenal-axis in patients with acute exacerbation of chronic obstructive pulmonary disease
Abstract
Background: As supra-physiological intake of corticosteroids is a well known risk factor for the development of adrenal insufficiency, we investigated the function of the hypothalamic-pituitary-adrenal (HPA) axis during a 14-day course of systemic corticosteroids in patients with acute exacerbation of chronic obstructive pulmonary disease using clinical and laboratory measures.
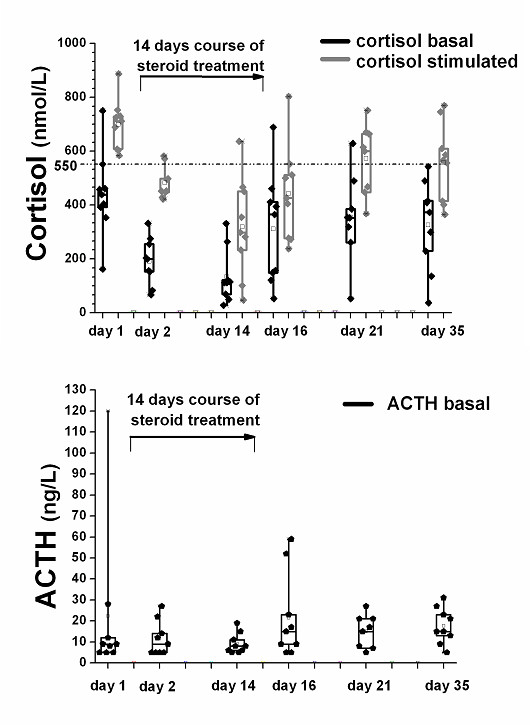
Methods: A systematic clinical and laboratory assessment including measurement of basal cortisol levels and the response to low dose (1 mug) ACTH stimulation was performed in nine patients before, on the first and the last day of treatment, as well as 2, 7 and 21 days after corticosteroid withdrawal.
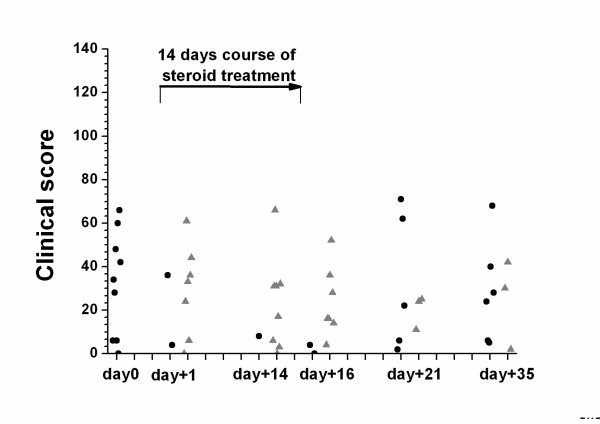
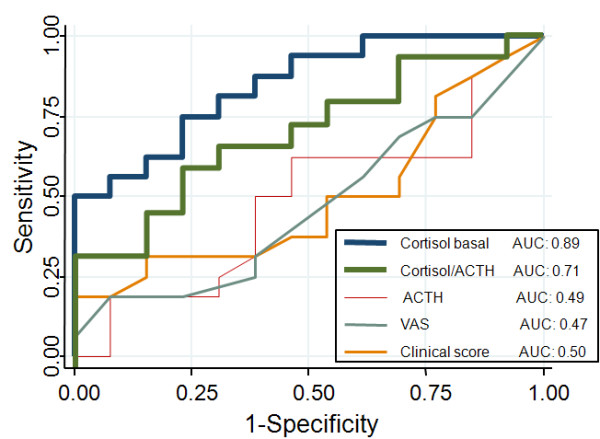
Results: At baseline, all nine patients had normal responses to 1 mug ACTH. On the first day of steroid treatment, 78% had a blunted peak cortisol response. This percentage increased to 89% after 14 days of steroid treatment. 78%, 33% and 33% of the patients had a blunted cortisol response to ACTH 2, 7, and 21 days after corticosteroid withdrawal, respectively. ROC curve analysis revealed that only basal cortisol concentrations (AUC 0.89), but not ACTH concentrations (AUC 0.49) or clinical signs (AUC 0.47) were predictive of an impaired function of the HPA axis. Basal cortisol levels of > 400 and < 150 nmol/l were 96% and 100% sensitive for a normal or pathological response to the ACTH stimulation test, respectively.
Conclusion: Immediate and prolonged suppression of the HPA axis is a common finding in otherwise asymptomatic patients undergoing systemic steroid treatment for acute exacerbation of chronic obstructive pulmonary disease and can reliably be assessed with the low-dose ACTH test.
Figures
References
-
- Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, Anderson P, Morgan NA. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999;340:1941–1947. doi: 10.1056/NEJM199906243402502. - DOI - PubMed
-
- Niewoehner DE. The role of systemic corticosteroids in acute exacerbation of chronic obstructive pulmonary disease. Am J Respir Med. 2002;1:243–248. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
