

Neuropsychological predictors of functional outcome in Cognitive Behavioral Social Skills Training for older people with schizophrenia
- PMID: 18222648
- PMCID: PMC2352154
- DOI: 10.1016/j.schres.2007.11.032
Neuropsychological predictors of functional outcome in Cognitive Behavioral Social Skills Training for older people with schizophrenia
Abstract
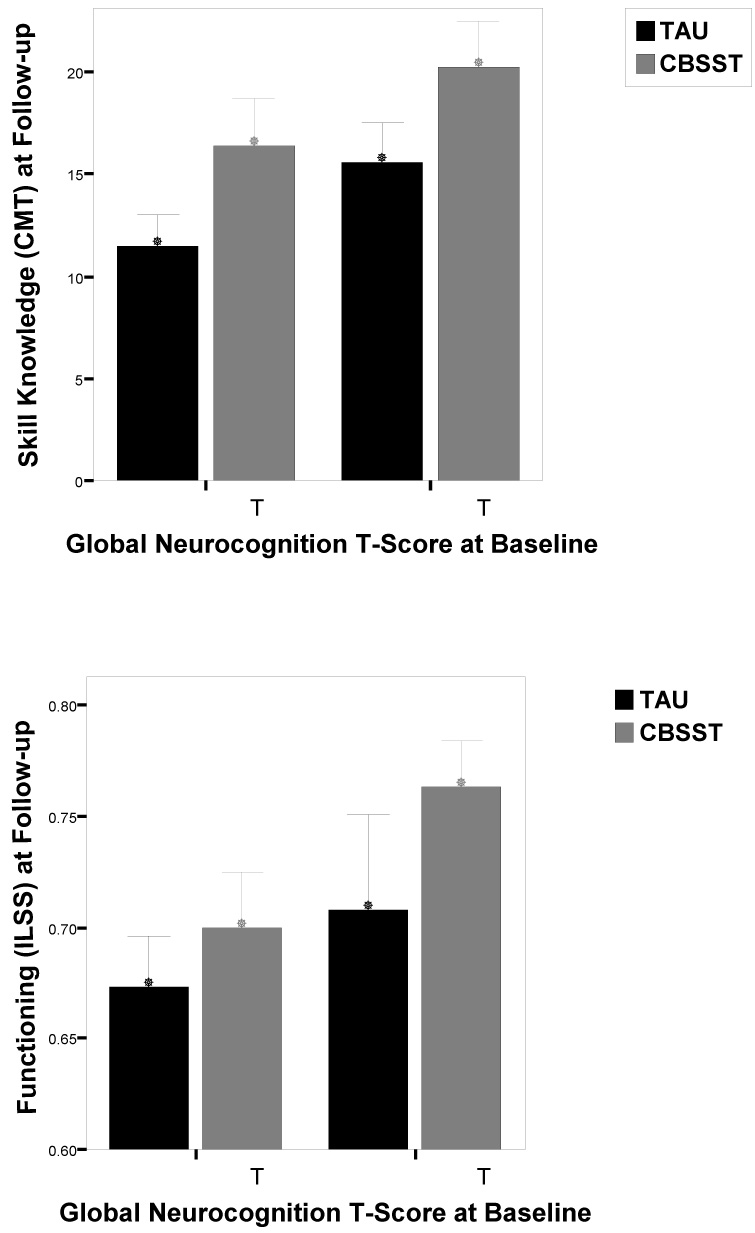
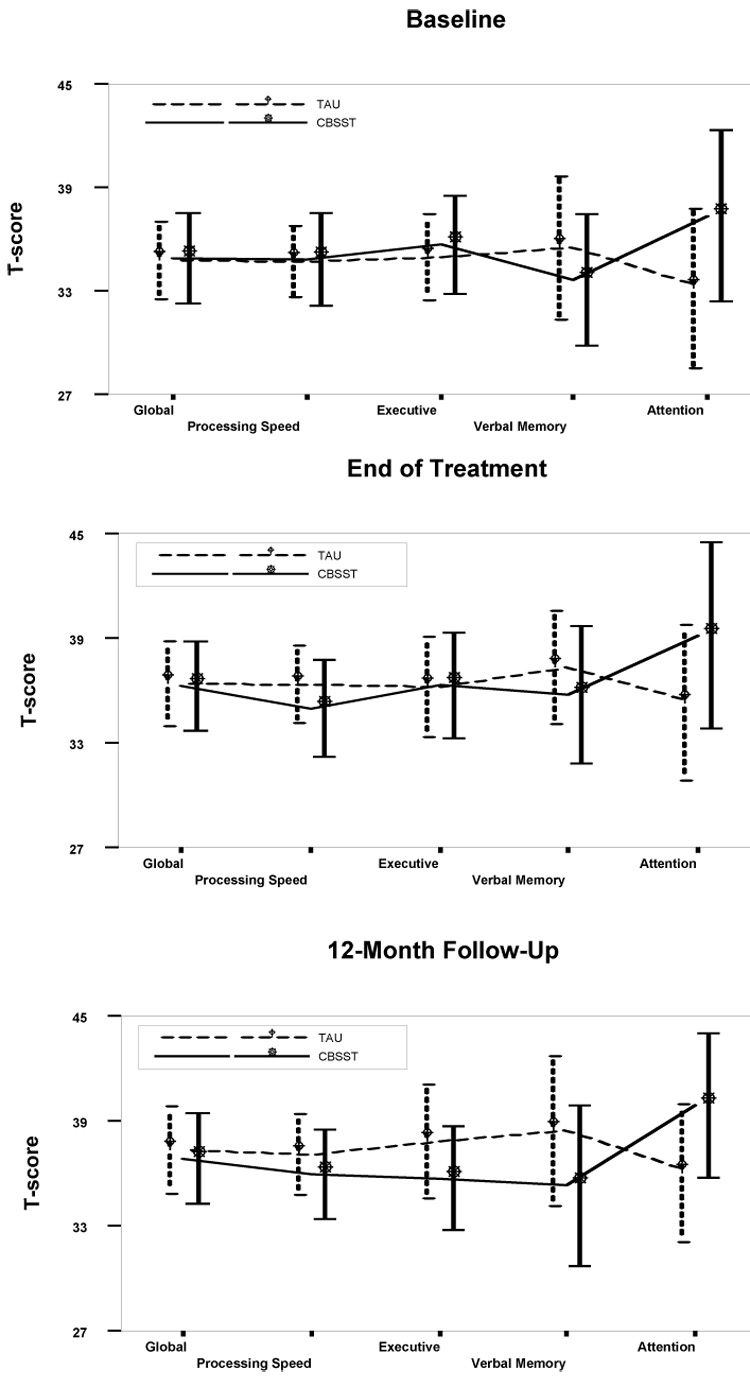
Cognitive Behavioral Social Skills Training (CBSST) is a 24-session weekly group therapy intervention to improve functioning in people with schizophrenia. In our prior randomized clinical trial comparing treatment as usual (TAU) with TAU plus group CBSST (Granholm, E., McQuaid, J.R., McClure, F.S., Auslander, L., Perivoliotis, D., Pedrelli, P., Patterson, T., Jeste, D.V., 2005. A randomized controlled trial of cognitive behavioral social skills training for middle-aged and older outpatients with chronic schizophrenia. Am. J. Psychiatry 162, 520-529.), participants with schizophrenia in CBSST showed significantly better functional outcome than participants in TAU. The present study was a secondary analysis of neuropsychological predictors of functional outcome in our prior CBSST trial. We examined (1) whether neuropsychological impairment at baseline moderated functional outcome in CBSST relative to TAU, and (2) whether improvement in neuropsychological abilities mediated improvement in functional outcome in CBSST. Attention, verbal learning/memory, speed of processing, and executive functions were assessed at baseline, end of treatment, and 12-month follow-up. Greater severity of neuropsychological impairment at baseline predicted poorer functional outcome for both treatment groups (nonspecific predictor), but the interaction between severity of neuropsychological impairment and treatment group was not significant (no moderation). Effect sizes for the difference between treatment groups on functional outcome measures at 12-month follow-up were similar for participants with relatively mild (d=.44-.64) and severe (d=.29-.60) neuropsychological impairment. Results also did not support the hypothesis that improvement in neuropsychological abilities mediated improvement in functioning in CBSST. Adding CBSST to standard pharmacologic care, therefore, improved functioning relative to standard care alone, even for participants with severe neuropsychological impairment, and this improvement in functioning was not related to improvement in neuropsychological abilities in CBSST.
Figures
References
-
- Asarnow RF, Granholm E, Sherman T. Span of apprehension in schizophrenia. In: Steinhauer SR, Gruzelier JH, Zubin J, editors. Handbook of Schizophrenia: Neurophsychology, Psychophysiology, and Information Processing. Amsterdam: Elsevier; 1991. pp. 335–370.
-
- Bartels SJ, Forester B, Mueser KT, Miles KM, Dums AR, Pratt SI, Sengupta A, Littlefield C, O'Hurley S, White P, Perkins L. Enhanced skills training and health care management for older persons with severe mental illness. Community Ment Health J. 2004;J. 40:75–90. - PubMed
-
- Beck AT, Rector NA. Cognitive therapy of schizophrenia: A new therapy for the new millennium. Am J Psychother. 2000;54:291–300. - PubMed
-
- Bowen L, Wallace CJ, Glynn SM, Nuechterlein KH, Lutzker J, Kuehnel TG. Schizophrenic individual's cognitive functioning and performance in interpersonal interactions and skills training procedures. J Psychiatr Res. 1994;28:289–301. - PubMed
-
- Bradshaw W. Integrating cognitive-behavioral psychotherapy for persons with schizophrenia into a psychiatric rehabilitation program: Results of a three year trial. Community Ment Health J. 2000;36:491–500. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
