

Conductive hearing loss caused by third-window lesions of the inner ear
- PMID: 18223508
- PMCID: PMC2577191
- DOI: 10.1097/mao.0b013e318161ab24
Conductive hearing loss caused by third-window lesions of the inner ear
Abstract
Background: Various authors have described conductive hearing loss (CHL), defined as an air-bone gap on audiometry, in patients without obvious middle ear pathologic findings. Recent investigations have suggested that many of these cases are due to disorders of the inner ear, resulting in pathologic third windows.
Objective: To provide an overview of lesions of the inner ear resulting in a CHL due to a third-window mechanism. The mechanism of the CHL is explained along with a classification scheme for these disorders. We also discuss methods for diagnosis of these disorders.
Data sources: The data were compiled from a review of the literature and recent published research on middle and inner ear mechanics from our laboratory.
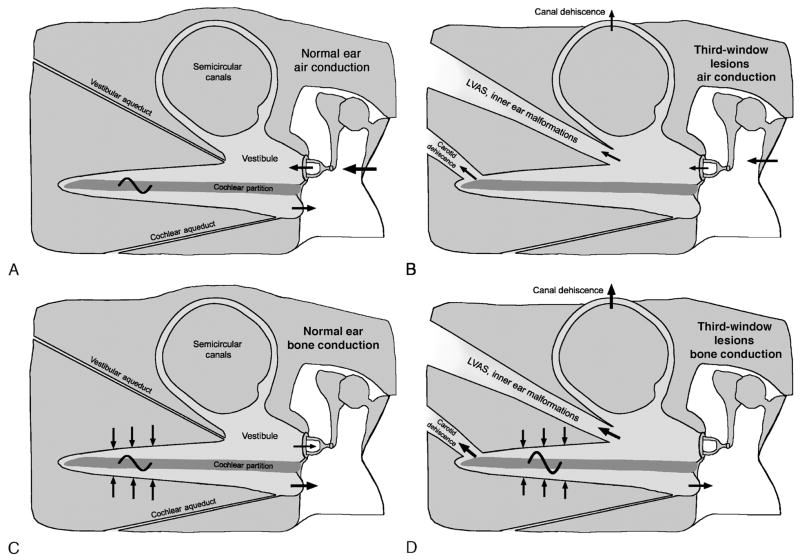
Conclusion: A number of disparate disorders affecting the labyrinth can produce CHL by acting as a pathologic third window in the inner ear. The common denominator is that these conditions result in a mobile window on the scala vestibuli side of the cochlear partition. The CHL results by the dual mechanism of worsening of air conduction thresholds and improvement of bone conduction thresholds. Such lesions may be anatomically discrete or diffuse. Anatomically discrete lesions may be classified by location: semicircular canals (superior, lateral, or posterior canal dehiscence), bony vestibule (large vestibular aqueduct syndrome, other inner ear malformations), or the cochlea (carotid-cochlear dehiscence, X-linked deafness with stapes gusher, etc.). An example of an anatomically diffuse lesion is Paget disease, which may behave as a distributed or diffuse third window. Third-window lesions should be considered in the differential diagnosis of CHL in patients with an intact tympanic membrane and an aerated, otherwise healthy, middle ear. Clues to suspect such a lesion include a low-frequency air-bone gap with supranormal thresholds for bone conduction, and presence of acoustic reflexes, vestibular evoked myogenic responses, or otoacoustic emission responses despite the CHL. Imaging studies can help confirm the diagnosis.
Figures
References
-
- Bess FH, Miller GW, Glasscock ME, Bratt GW. Unexplained conductive hearing loss. South Med J. 1980;73:335–8. - PubMed
-
- House JW, Sheehy JL, Antunez JC. Stapedectomy in children. Laryngoscope. 1980;90:1804–9. - PubMed
-
- Al Muhaimeed H, El Sayed Y, Rabah A, Al-Essa A. Conductive hearing loss: investigation of possible inner ear origin in three cases studies. J Laryngol Otol. 2002;116:942–5. - PubMed
-
- Schuknecht HF. Otologic mystery. Am J Otol. 1987;8:182–3. - PubMed
-
- Snik AF, Hombergen GC, Mylanus EA, Cremers CW. Air-bone gap in patients with X-linked stapes gusher syndrome. Am J Otol. 1995;16:241–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
