

Clinical outcomes by race in hypertensive patients with and without the metabolic syndrome: Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
- PMID: 18227370
- PMCID: PMC2805022
- DOI: 10.1001/archinternmed.2007.66
Clinical outcomes by race in hypertensive patients with and without the metabolic syndrome: Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)
Abstract
Background: Antihypertensive drugs with favorable metabolic effects are advocated for first-line therapy in hypertensive patients with metabolic/cardiometabolic syndrome (MetS). We compared outcomes by race in hypertensive individuals with and without MetS treated with a thiazide-type diuretic (chlorthalidone), a calcium channel blocker (amlodipine besylate), an alpha-blocker (doxazosin mesylate), or an angiotensin-converting enzyme inhibitor (lisinopril).
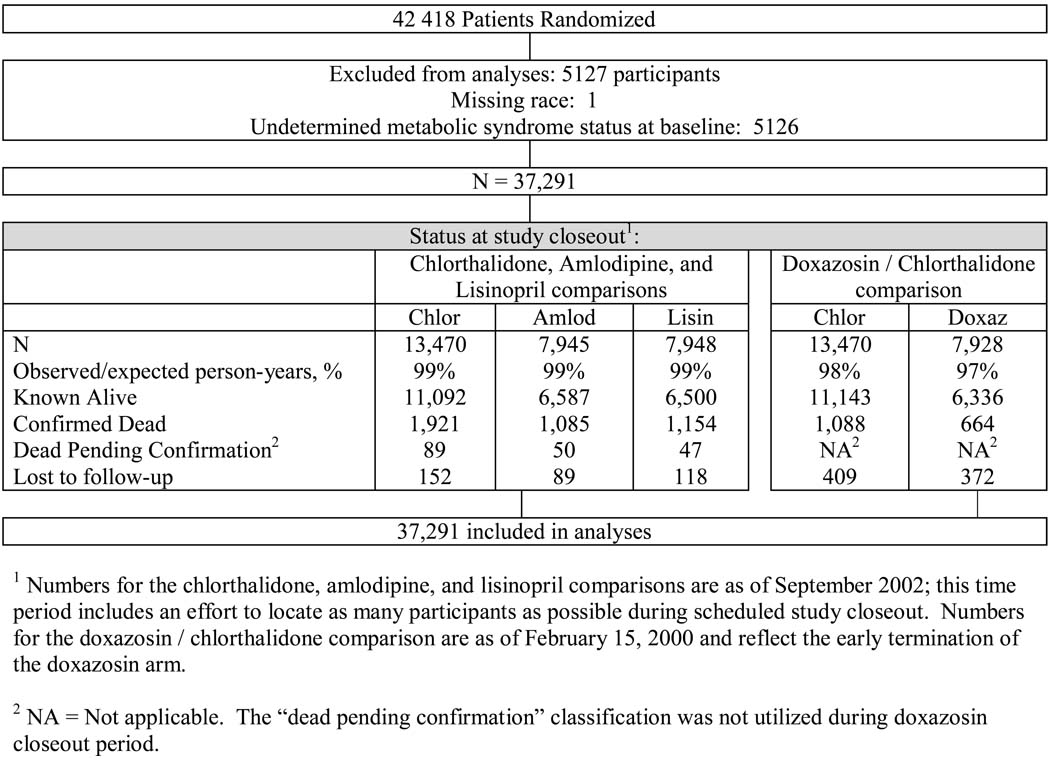
Methods: A subgroup analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), a randomized, double-blind hypertension treatment trial of 42 418 participants. We defined MetS as hypertension plus at least 2 of the following: fasting serum glucose level of at least 100 mg/dL, body mass index (calculated as weight in kilograms divided by height in meters squared) of at least 30, fasting triglyceride levels of at least 150 mg/dL, and high-density lipoprotein cholesterol levels of less than 40 mg/dL in men or less than 50 mg/dL in women.
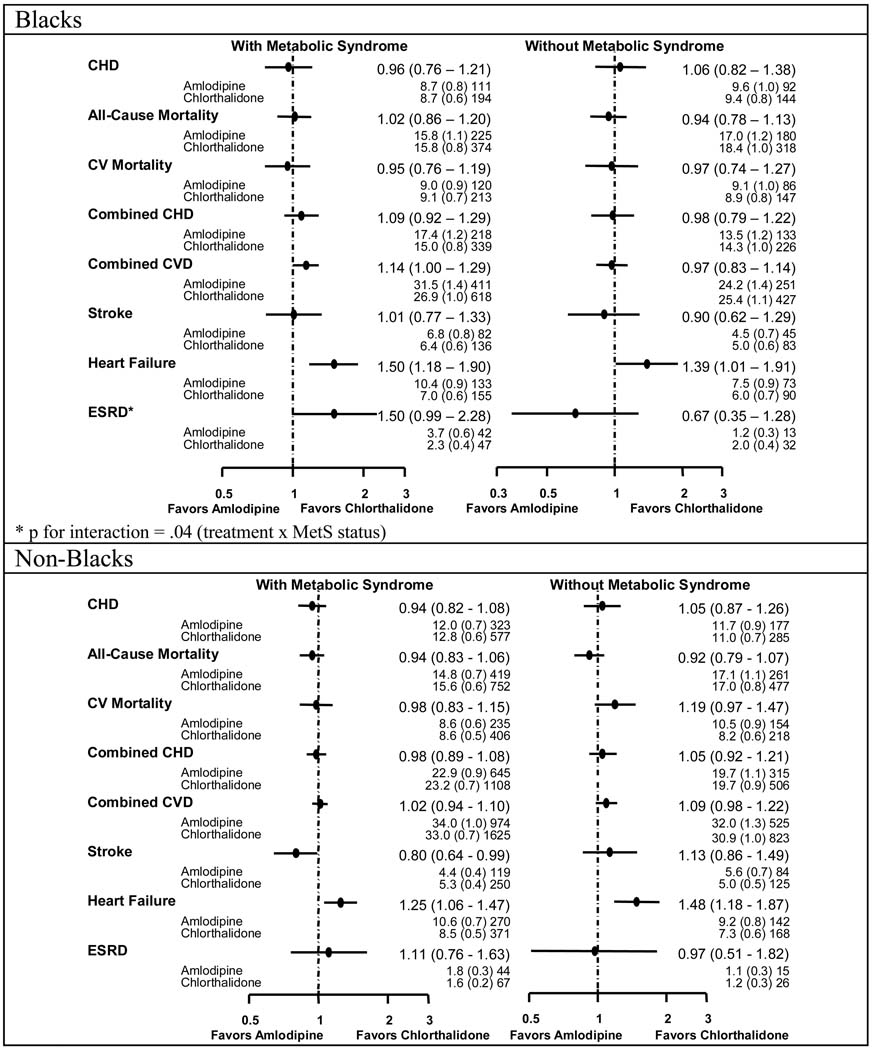
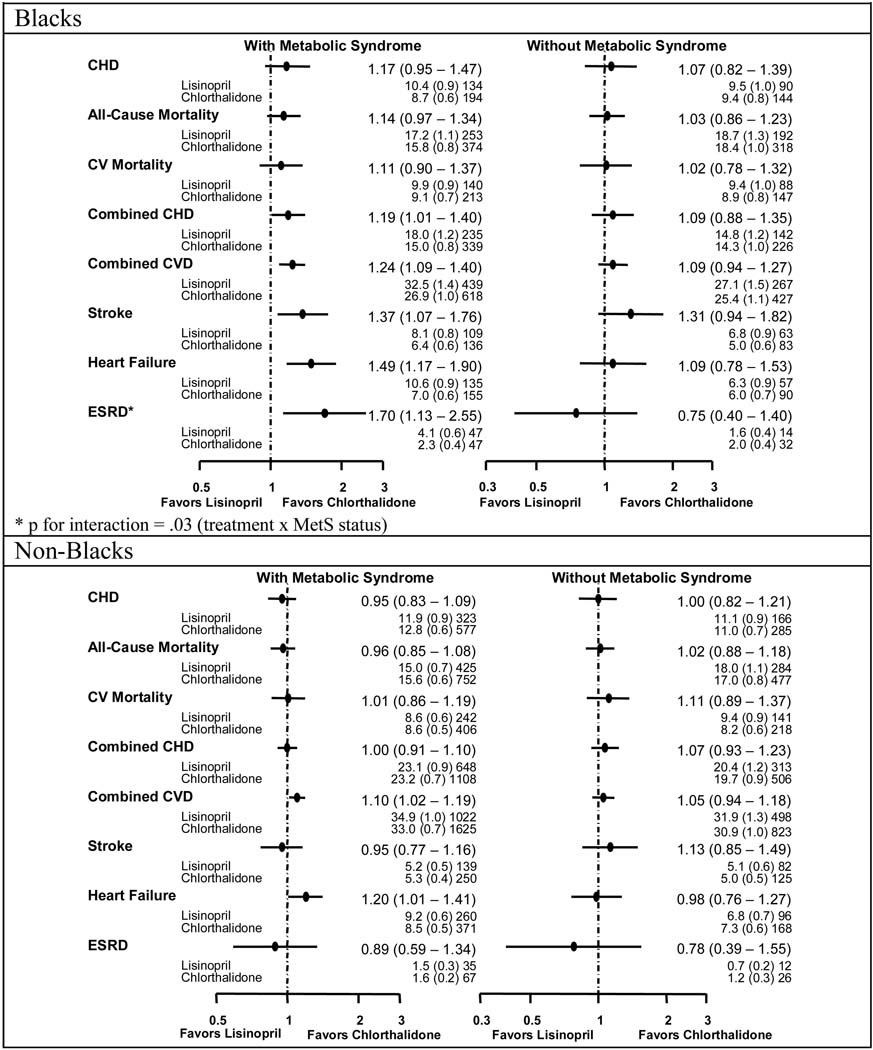
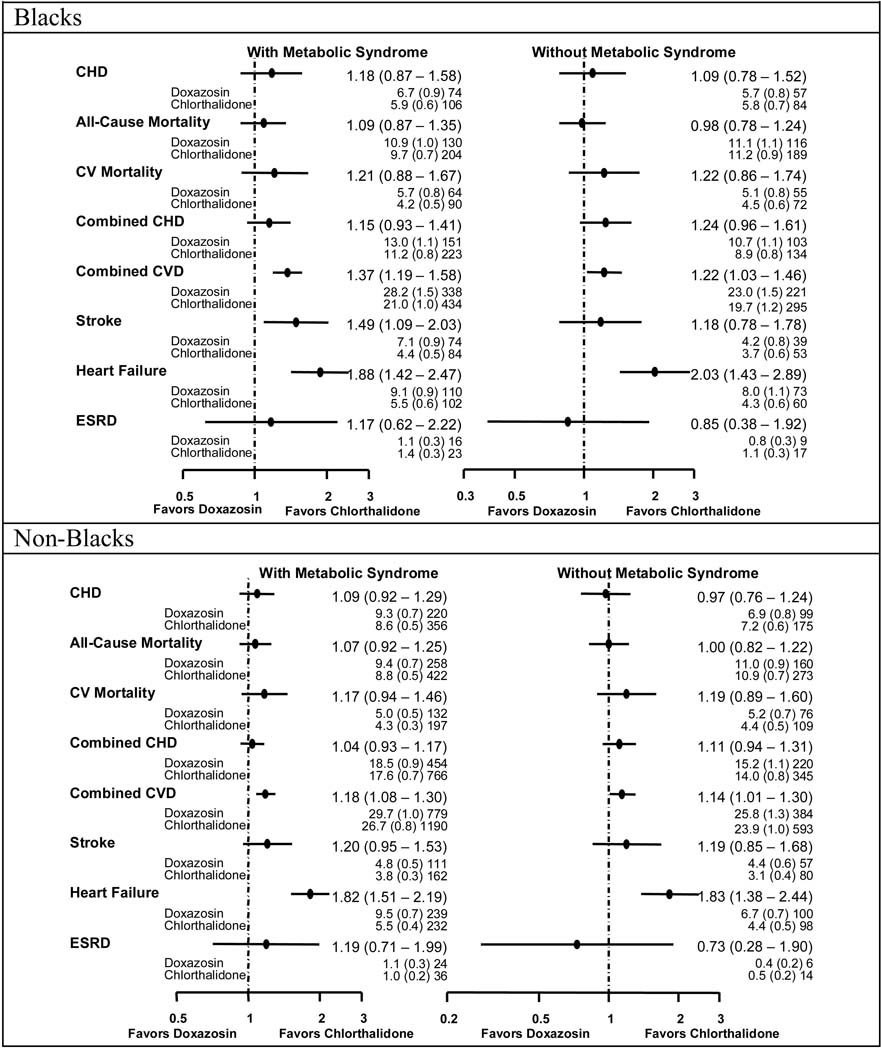
Results: Significantly higher rates of heart failure were consistent across all treatment comparisons in those with MetS. Relative risks (RRs) were 1.50 (95% confidence interval, 1.18-1.90), 1.49 (1.17-1.90), and 1.88 (1.42-2.47) in black participants and 1.25 (1.06-1.47), 1.20 (1.01-1.41), and 1.82 (1.51-2.19) in nonblack participants for amlodipine, lisinopril, and doxazosin comparisons with chlorthalidone, respectively. Higher rates for combined cardiovascular disease were observed with lisinopril-chlorthalidone (RRs, 1.24 [1.09-1.40] and 1.10 [1.02-1.19], respectively) and doxazosin-chlorthalidone comparisons (RRs, 1.37 [1.19-1.58] and 1.18 [1.08-1.30], respectively) in black and nonblack participants with MetS. Higher rates of stroke were seen in black participants only (RR, 1.37 [1.07-1.76] for the lisinopril-chlorthalidone comparison, and RR, 1.49 [1.09-2.03] for the doxazosin-chlorthalidone comparison). Black patients with MetS also had higher rates of end-stage renal disease (RR, 1.70 [1.13-2.55]) with lisinopril compared with chlorthalidone.
Conclusions: The ALLHAT findings fail to support the preference for calcium channel blockers, alpha-blockers, or angiotensin-converting enzyme inhibitors compared with thiazide-type diuretics in patients with the MetS, despite their more favorable metabolic profiles. This was particularly true for black participants.
Trial registration: ClinicalTrials.gov NCT00000542.
Figures
Comment in
-
Hypertension with metabolic syndrome: think thiazides are old hat? ALLHAT says think again.J Fam Pract. 2008 May;57(5):306-10. J Fam Pract. 2008. PMID: 18460295 Free PMC article.
References
-
- Hall WD, Clark LT, Wenger NK, Wright JT, Jr., Kumanyika SK, Watson K, et al. The Metabolic Syndrome in African Americans: a review. Ethn Dis. 2003;13(4):414–428. - PubMed
-
- Grundy SM, Brewer HB, Jr., Cleeman JI, Smith SC, Jr., Lenfant C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109(3):433–438. - PubMed
-
- Eckel RH, Kahn R, Robertson RM, Rizza RA. Preventing cardiovascular disease and diabetes: a call to action from the American Diabetes Association and the American Heart Association. Circulation. 2006;113(25):2943–2946. - PubMed
-
- Mykkanen L, Kuusisto J, Pyorala K, Laakso M, Haffner SM. Increased risk of non-insulin-dependent diabetes mellitus in elderly hypertensive subjects. J Hypertens. 1994;12(12):1425–1432. - PubMed
