

Alpha blockers for the treatment of benign prostatic hyperplasia
- PMID: 18231614
- PMCID: PMC2213889
Alpha blockers for the treatment of benign prostatic hyperplasia
Abstract
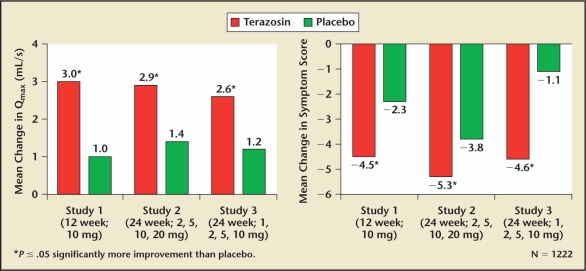
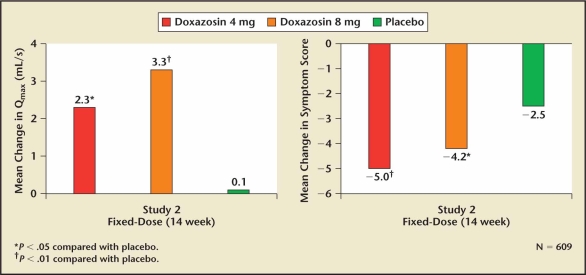
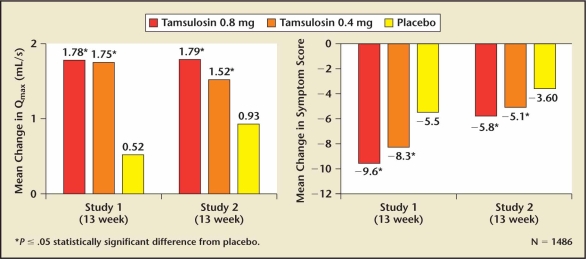
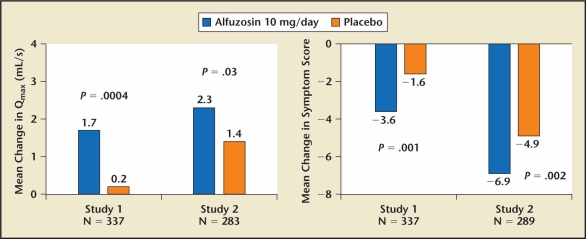
The evolution of alpha blocker therapy for benign prostatic hyperplasia (BPH) has focused on improving convenience and tolerability. Indications for treating BPH include reversing signs and symptoms or preventing progression of the disease. The indication that most commonly drives the need for intervention is relief of lower urinary tract symptoms (LUTS) with the intent of improving quality of life. Alpha blockers are the most effective, least costly, and best tolerated of the drugs for relieving LUTS. Four long-acting alpha 1 blockers are approved by the Food and Drug Administration for treatment of symptomatic LUTS/BPH: terazosin, doxazosin, tamsulosin, and alfuzosin. All are well tolerated and have comparable dose-dependent effectiveness. Tamsulosin and alfuzosin SR do not require dose titration. Alfuzosin, terazosin, and doxazosin have all been shown to be effective in relieving LUTS/BPH independent of prostate size.
Keywords: Alfuzosin; Alpha blockers; Benign prostatic hyperplasia; Doxazosin; Lower urinary tract symptoms; Quality of life; Tamsulosin; Terazosin.
Figures
Similar articles
-
α-Blockers for benign prostatic hyperplasia: the new era.Curr Opin Urol. 2012 Jan;22(1):7-15. doi: 10.1097/MOU.0b013e32834d9bfd. Curr Opin Urol. 2012. PMID: 22080875 Review.
-
The evolution of alpha-blockers for the treatment of benign prostatic hyperplasia.Rev Urol. 2006;8 Suppl 4(Suppl 4):S3-9. Rev Urol. 2006. PMID: 17215999 Free PMC article.
-
A meta-analysis on the efficacy and tolerability of alpha1-adrenoceptor antagonists in patients with lower urinary tract symptoms suggestive of benign prostatic obstruction.Eur Urol. 1999;36(1):1-13. doi: 10.1159/000019919. Eur Urol. 1999. PMID: 10364649
-
A randomized, comparative, open-label study of efficacy and tolerability of alfuzosin, tamsulosin and silodosin in benign prostatic hyperplasia.Indian J Pharmacol. 2016 Mar-Apr;48(2):134-40. doi: 10.4103/0253-7613.178825. Indian J Pharmacol. 2016. PMID: 27127315 Free PMC article. Clinical Trial.
-
The diagnosis and treatment of lower urinary tract symptoms due to benign prostatic hyperplasia with α-blockers: focus on silodosin.Clin Drug Investig. 2015 Feb;35 Suppl 1:7-18. doi: 10.1007/s40261-014-0257-3. Clin Drug Investig. 2015. PMID: 25708606 Review.
Cited by
-
Association between Bladder Outlet Obstruction and Bladder Cancer in Patients with Aging Male.J Clin Med. 2019 Sep 27;8(10):1550. doi: 10.3390/jcm8101550. J Clin Med. 2019. PMID: 31569597 Free PMC article.
-
Identification of repurposable drugs with beneficial effects on glucose control in type 2 diabetes using machine learning.Pharmacol Res Perspect. 2019 Nov 20;7(6):e00529. doi: 10.1002/prp2.529. eCollection 2019 Dec. Pharmacol Res Perspect. 2019. PMID: 31763043 Free PMC article.
-
The use of 5-alpha reductase inhibitors in the treatment of benign prostatic hyperplasia.Asian J Urol. 2018 Jan;5(1):28-32. doi: 10.1016/j.ajur.2017.11.005. Epub 2017 Nov 26. Asian J Urol. 2018. PMID: 29379733 Free PMC article. Review.
-
Pharmacokinetic bioequivalence studies of a fixed-dose combination of tamsulosin and dutasteride in healthy volunteers.Clin Drug Investig. 2014 May;34(5):335-49. doi: 10.1007/s40261-014-0179-0. Clin Drug Investig. 2014. PMID: 24615171 Clinical Trial.
-
The residual nonadrenergic contractile response to nerve stimulation of the mouse prostate is mediated by acetylcholine but not ATP in a comparison with the mouse vas deferens.J Pharmacol Exp Ther. 2010 Nov;335(2):489-96. doi: 10.1124/jpet.110.172130. Epub 2010 Aug 19. J Pharmacol Exp Ther. 2010. PMID: 20724483 Free PMC article.
References
-
- McNeal JG. The prostate gland: morphology and pathobiology. Monogr Urol. 1983;4:3–33.
-
- Berry SJ, Coffey DS, Walsh PC, et al. The development of human prostatic hyperplasia with age. J Urol. 1984;132:474–479. - PubMed
-
- Girman CJ, Jacobsen SJ, Guess HA, et al. Natural history of prostatism: relationship among symptoms, prostate volume and peak urinary flow rate. J Urol. 1995;153:1510–1515. - PubMed
-
- Lepor H. The pathophysiology of lower urinary tract symptoms in the aging male population. In: Lepor H, editor. Prostatic Diseases. Philadelphia, PA: WB Saunders; 2000. pp. 163–196.
-
- Jepsen JB, Bruskewitz RC. Clinical manifestations and indications for treatment. In: Lepor H, editor. Prostatic Diseases. Philadelphia, PA: WB Saunders; 2000. pp. 127–142.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials