

The NIH registry on use of the Wingspan stent for symptomatic 70-99% intracranial arterial stenosis
- PMID: 18235078
- PMCID: PMC3506389
- DOI: 10.1212/01.wnl.0000306308.08229.a3
The NIH registry on use of the Wingspan stent for symptomatic 70-99% intracranial arterial stenosis
Abstract
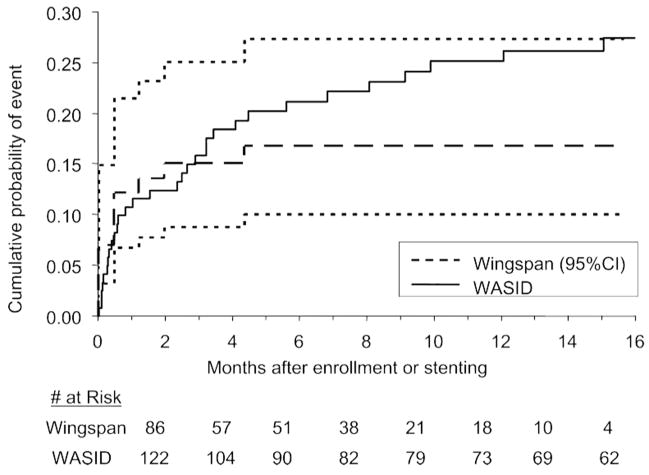
Background: The Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) trial showed that patients with symptomatic 70% to 99% intracranial arterial stenosis are at particularly high risk of ipsilateral stroke on medical therapy: 18% at 1 year (95% CI = 3% to 24%). The Wingspan intracranial stent is another therapeutic option but there are limited data on the technical success of stenting and outcome of patients with 70% to 99% stenosis treated with a Wingspan stent.
Methods: Sixteen medical centers enrolled consecutive patients treated with a Wingspan stent in this registry between November 2005 and October 2006. Data on stenting indication, severity of stenosis, technical success (stent placement across the target lesion with <50% residual stenosis), follow-up angiography, and outcome were collected.
Results: A total of 129 patients with symptomatic 70% to 99% intracranial stenosis were enrolled. The technical success rate was 96.7%. The mean pre and post-stent stenoses were 82% and 20%. The frequency of any stroke, intracerebral hemorrhage, or death within 30 days or ipsilateral stroke beyond 30 days was 14.0% at 6 months (95% CI = 8.7% to 22.1%). The frequency of >or=50% restenosis on follow-up angiography was 13/52 (25%).
Conclusion: The use of a Wingspan stent in patients with severe intracranial stenosis is relatively safe with high rate of technical success with moderately high rate of restenosis. Comparison of the event rates in high-risk patients in Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) vs this registry do not rule out either that stenting could be associated with a substantial relative risk reduction (e.g., 50%) or has no advantage compared with medical therapy. A randomized trial comparing stenting with medical therapy is needed.
Figures


Comment in
-
Registries: they're not just for weddings anymore.Neurology. 2008 Apr 22;70(17):1508-9. doi: 10.1212/01.wnl.0000308705.27951.c2. Epub 2008 Jan 30. Neurology. 2008. PMID: 18235077 No abstract available.
-
The NIH registry on use of the Wingspan stent for symptomatic 70-99% intracranial arterial stenosis.Neurology. 2008 Sep 30;71(14):1124; author reply 1124-5. doi: 10.1212/01.wnl.000032353.550765.3c. Neurology. 2008. PMID: 18824679 No abstract available.
References
-
- Wityk RJ, Lehman D, Klag M, Coresh J, Ahn H, Litt B. Race and sex differences in the distribution of cerebral atherosclerosis. Stroke. 1996;27:1974–1980. - PubMed
-
- Sacco RL, Kargman DE, Gu Q, Zamanillo MC. Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction: The Northern Manhattan stroke study. Stroke. 1995;26:14–20. - PubMed
-
- Wong KS, Huang YN, Gao S, Lam WW, Chan YL, Kay R. Intracranial stenosis in Chinese patients with acute stroke. Neurology. 1998;50:812–813. - PubMed
-
- Feldmann E, Daneult N, Kwan E, et al. Chinese-white differences in the distribution of occlusive cerebrovascular disease. Neurology. 1990;40:1541–1545. - PubMed
-
- Broderick J, Brott T, Kothari R, et al. The Greater Cincinnati/Northern Kentucky Stroke Study: preliminary first ever and total incidence rates of stroke among black. Stroke. 1998;29:415–421. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical