

Antibody-mediated rejection of the kidney after simultaneous pancreas-kidney transplantation
- PMID: 18235091
- PMCID: PMC2390970
- DOI: 10.1681/ASN.2007070736
Antibody-mediated rejection of the kidney after simultaneous pancreas-kidney transplantation
Abstract
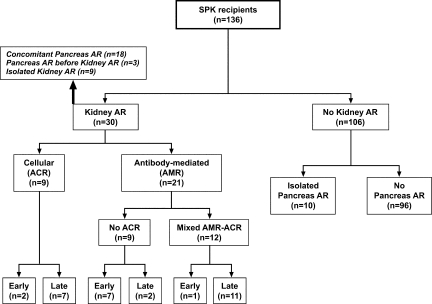
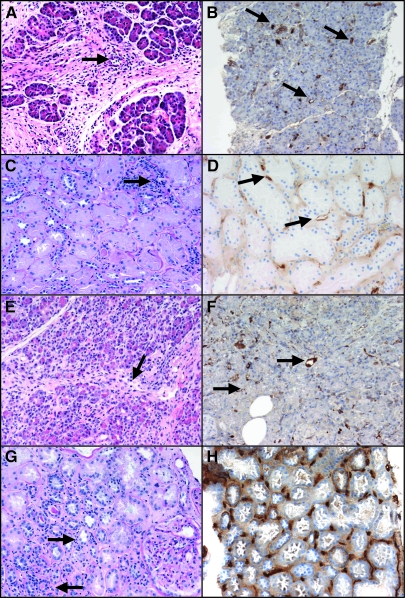
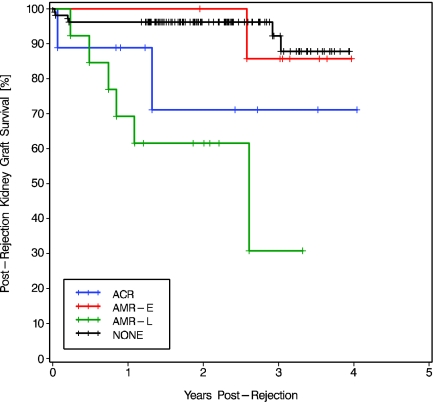
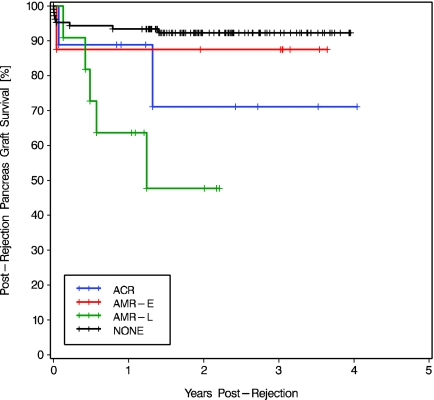
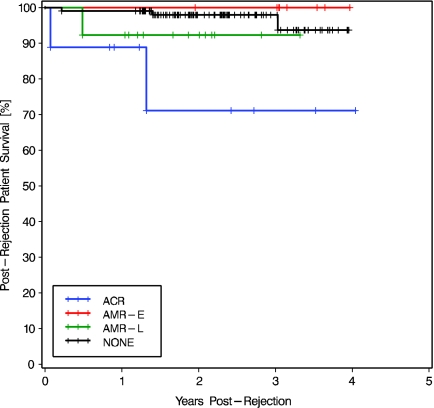
The prevalence, risk factors, and outcome of antibody-mediated rejection (AMR) of the kidney after simultaneous pancreas-kidney transplantation are unknown. In 136 simultaneous pancreas-kidney recipients who were followed for an average of 3.1 yr, 21 episodes of AMR of the kidney allograft were identified. Eight episodes occurred early (</=90 d) after transplantation, and 13 occurred later. Histologic evidence of concomitant acute cellular rejection was noted in 12 cases; the other nine had evidence only of humoral rejection. In 13 cases, clinical rejection of the pancreas was diagnosed simultaneously, and two of these were biopsy proven and were positive for C4d immunostaining. Multivariate analysis identified only one significant risk factor: Female patients were three times more likely to experience AMR. Nearly all early episodes resolved with treatment and did not predict graft loss, but multivariate Cox models revealed that late AMR episodes more than tripled the risk for kidney and pancreas graft loss; therefore, new strategies are needed to prevent and to treat late AMR in simultaneous pancreas-kidney transplant recipients.
Figures
References
-
- Rayhill SC, D'Alessandro AM, Odorico JS, Knechtle SJ, Pirsch JD, Heisey DM, Kirk AD, Van der Werf W, Sollinger HW: Simultaneous pancreas-kidney transplantation and living related donor renal transplantation in patients with diabetes: Is there a difference in survival? Ann Surg 231: 417–423, 2000 - PMC - PubMed
-
- Di Carlo A, Odorico JS, Leverson GE, Fernandez LA, Chin LT, Becker YT, Knechtle SJ, Pirsch JD, D'Alessandro AM, Sollinger HW. Long-term outcomes in simultaneous pancreas-kidney transplantation: Lessons relearned. Clin Transpl 215–220, 2003 - PubMed
-
- Fernandez LA, Di Carlo A, Odorico JS, Leverson GE, Shames BD, Becker YT, Chin LT, Pirsch JD, Knechtle SJ, Foley DP, Sollinger HW, D'Alessandro AM: Simultaneous pancreas-kidney transplantation from donation after cardiac death: Successful long-term outcomes. Ann Surg 242: 716–723, 2005 - PMC - PubMed
-
- Salvalaggio PR, Schnitzler MA, Abbott KC, Brennan DC, Irish W, Takemoto SK, Axelrod D, Santos LS, Kocak B, Willoughby L, Lentine KL: Patient and graft survival implications of simultaneous pancreas kidney transplantation from old donors. Am J Transplant 7: 1561–1571, 2007 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
