

Retrospective review of the frequency of ECG changes in hyperkalemia
- PMID: 18235147
- PMCID: PMC2390954
- DOI: 10.2215/CJN.04611007
Retrospective review of the frequency of ECG changes in hyperkalemia
Abstract
Background and objectives: Experimentally elevated potassium causes a clear pattern of electrocardiographic changes, but, clinically, the reliability of this pattern is unclear. Case reports suggest patients with renal insufficiency may have no electrocardiographic changes despite markedly elevated serum potassium. In a prospective series, 46% of patients with hyperkalemia were noted to have electrocardiographic changes, but no clear criteria were presented.
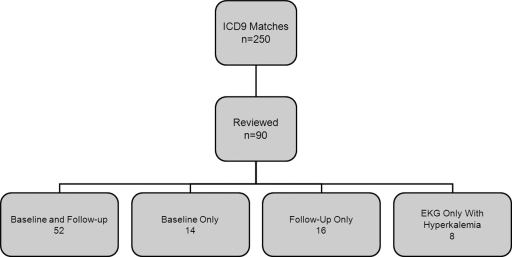
Design, setting, participants, & measurements: Charts were reviewed for patients who were admitted to a community-based hospital with a diagnosis of hyperkalemia. Inclusion criteria were potassium >/=6 with a concurrent electrocardiogram. Data were abstracted regarding comorbid diagnoses, medications, and treatment. Potassium concentrations were documented along with other electrolytes, pH, creatinine, and biomarkers of cardiac injury. Coincident, baseline, and follow-up electrocardiograms were examined for quantitative and qualitative changes in the QRS and T waves as well as the official cardiology readings.
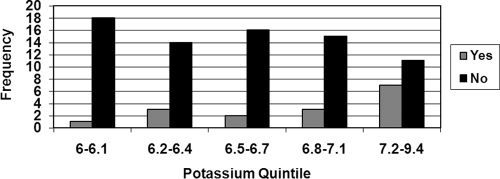
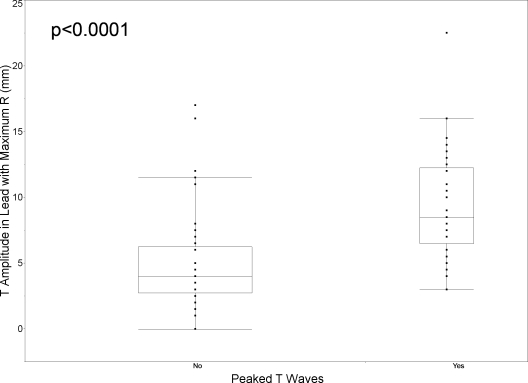
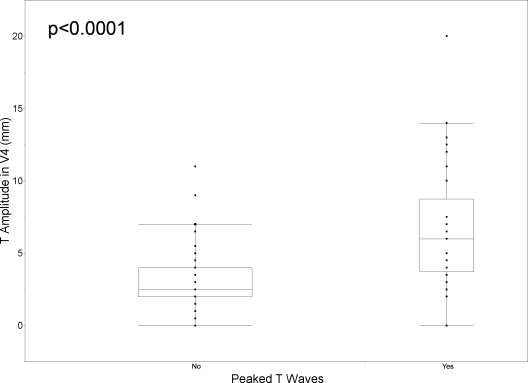
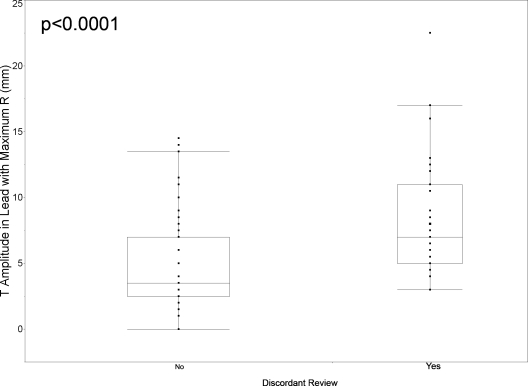
Results: Ninety patients met criteria; two thirds were older than 65, and 48% presented with renal failure. Common medications included beta blockers, insulin, and aspirin; 80% had potassium <7.2. The electrocardiogram was insensitive for diagnosing hyperkalemia. Quantitative assessments of T-wave amplitude corroborated subjective assessments of T-wave peaking; however, no diagnostic threshold could be established. The probability of electrocardiographic changes increased with increasing potassium. The correlation between readers was moderate.
Conclusions: Given the poor sensitivity and specificity of electrocardiogram changes, there is no support for their use in guiding treatment of stable patients. Without identifiable electrocardiographic markers of the risk for complications, management of hyperkalemia should be guided by the clinical scenario and serial potassium measurements.
Figures
References
-
- Moore M, Bailery R: Incidence of hyperkalemia in hospitalized patients. N Z Med J 102: 557–558, 1989 - PubMed
-
- Shemer J, Modan M, Ezra D, Cabili S: Incidence of hyperkalemia in hospitalized patients. Isr J Med Sci 19: 659–661, 1983 - PubMed
-
- Borra S, Shaker R, Kleinfeld M: Hyperkalemia in an adult hospitalized population. Mt Sinai J Med 55: 226–229, 1988 - PubMed
-
- Oster J, Singer I, Fishman L: Heparin-induced aldosterone suppression and hyperkalemia. Am J Med 98: 575–586, 1995 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
